
Stopping Wellbutrin often starts with a simple thought. The medication helped at one point, but now the side effects feel frustrating, life circumstances have changed, or another treatment plan is on the table. That moment can bring relief, but it also brings a lot of uncertainty.
Individuals searching for a Wellbutrin taper schedule don't just want a list of dose changes. They want to know what's safe, what's overhyped, what can go wrong, and when tapering at home stops being a reasonable option. That distinction matters, especially for anyone with a seizure history, substance use, bipolar symptoms, or multiple psychiatric medications.
This is not a do-it-yourself stop guide. It's a clinician's framework for the conversation that needs to happen with a prescriber, and in higher-risk situations, with a supervised treatment team.
Why a Careful Wellbutrin Taper Is So Important
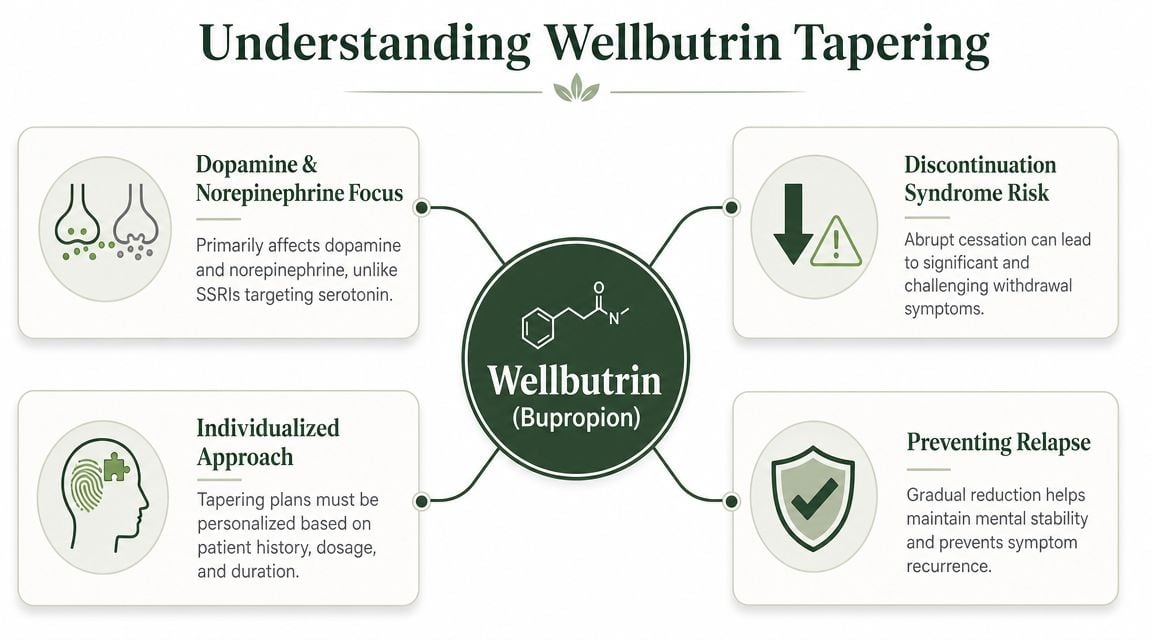
Wellbutrin is bupropion, and it isn't an SSRI. That difference shapes how clinicians think about stopping it.
Historically, bupropion was treated differently from many other antidepressants because the early evidence did not show a general withdrawal syndrome that required routine tapering. A NIH-indexed review of clinical trial and postmarketing data stated that “the evidence does not indicate that bupropion is associated with withdrawal symptoms” and “does not support a general recommendation to taper the dose” before stopping, in the context of a medication that has been used as an antidepressant for over 20 years (NIH-indexed review of bupropion discontinuation history).
That history matters because patients still hear mixed messages. Some are told bupropion has “no withdrawal.” Others are told every antidepressant must be tapered the same way. Neither statement is precise enough for real-world care.
Why the distinction still matters
A patient can feel worse after lowering Wellbutrin for at least two very different reasons:
- Medication discontinuation effects can show up as a temporary adjustment problem after a dose drop.
- Relapse means the original depression, low motivation, or other target symptoms are returning.
- Medication switch effects can add confusion if another antidepressant or mood medication is being started or changed at the same time.
These situations can look similar in the first few days. That's why a safe plan isn't just about reducing pills. It's about knowing what the medication was treating, what symptoms were present before treatment, and what pattern would signal trouble.
A taper isn't only about preventing discomfort. It also helps separate temporary adjustment from the return of the condition being treated.
What careful tapering actually does
A thoughtful Wellbutrin taper schedule gives the brain and the patient time to respond to change in a controlled way. It also gives the prescriber time to answer practical questions:
- Is the person stopping because of side effects, remission, or a treatment transition?
- Did the patient improve on Wellbutrin in ways they may not fully appreciate until the dose drops?
- Are appetite, energy, sleep, and mood likely to change in ways that could be misread?
Those questions are especially important for people already monitoring weight, appetite, and mood together. For a broader patient-friendly discussion of that overlap, this resource on understanding weight loss and well-being can help frame why medication changes sometimes affect more than mood alone.
The practical takeaway
Wellbutrin discontinuation deserves nuance. It isn't usually approached with the same assumptions used for serotonin-based antidepressants, but that doesn't mean stopping it should be casual. In current practice, tapering is often guided by dose, formulation, symptom history, and risk profile rather than by a blanket rule.
Key Factors That Define Your Tapering Plan
No prescriber should hand out the same Wellbutrin taper schedule to every patient. Safe tapering depends on the medication itself, the person taking it, and the reason for stopping.
The medication variables that matter
The first part of the conversation is simple and concrete.
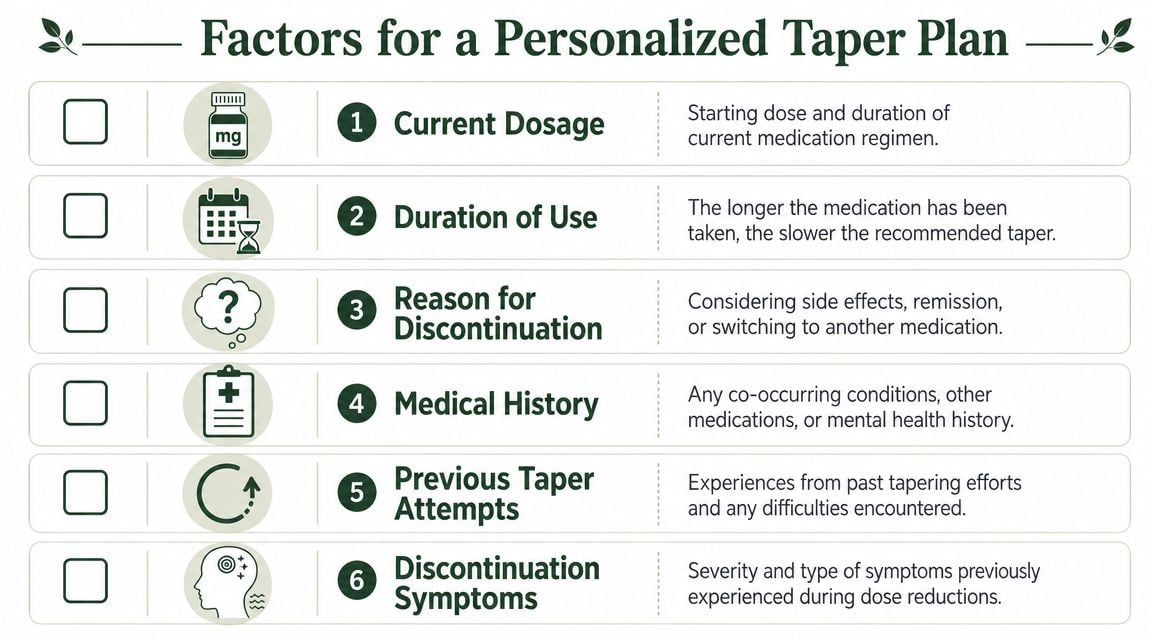
- Current dose matters. A person taking a higher daily dose usually needs a more deliberate step-down than someone already at a lower strength.
- Formulation matters. SR and XL behave differently in the body and create different practical taper options.
- Duration of treatment matters. Someone who has taken bupropion for a short period may have a smoother discontinuation than someone who has relied on it for a long time.
- Reason for discontinuation matters. Stopping because of anxiety, insomnia, appetite change, or a switch to another medication creates different clinical priorities.
Dose consistency also matters more than many patients realize. Missed doses can mimic early taper symptoms and make the picture confusing. For readers trying to build better medication routines before discussing a taper, it may help to learn about dose consistency with PepFlow.
The personal risk factors your doctor needs to know
This is the part patients sometimes minimize. They shouldn't.
A prescriber needs a full picture of psychiatric history, substance use, seizure risk, eating disorder history, and prior taper attempts. If any of that information is incomplete, the taper plan may look safer on paper than it is in real life.
Here are the issues that usually change the plan:
Past problems during medication changes
If previous dose reductions caused agitation, insomnia, mood drops, or confusion, the next taper should be slower and more closely monitored.Co-occurring mental health conditions
Depression alone is one thing. Depression with panic symptoms, trauma symptoms, bipolar features, or obsessive thinking is another.Other medications and substances
Alcohol, sedatives, stimulants, and multiple psychiatric prescriptions can all complicate what looks like a straightforward dose reduction.
Bring a written medication list to the taper visit. Include prescriptions, supplements, alcohol use patterns, and any “as needed” medications. That's often where hidden risk shows up.
Questions worth asking before any dose change
A strong appointment usually includes direct questions like these:
- What symptoms should be tracked between dose reductions?
- What would count as a normal adjustment versus a reason to pause?
- Is the current formulation the easiest one to taper safely?
- If symptoms show up, should the patient hold the current dose or call first?
- What would make medical supervision necessary?
A good taper plan is individualized before the first pill changes, not improvised after symptoms appear.
Sample Wellbutrin Taper Schedules for Discussion
Patients usually want examples, and that's reasonable. Seeing a sample taper makes the process feel less mysterious. But examples are not prescriptions, and copying someone else's Wellbutrin taper schedule without medical review is a mistake.
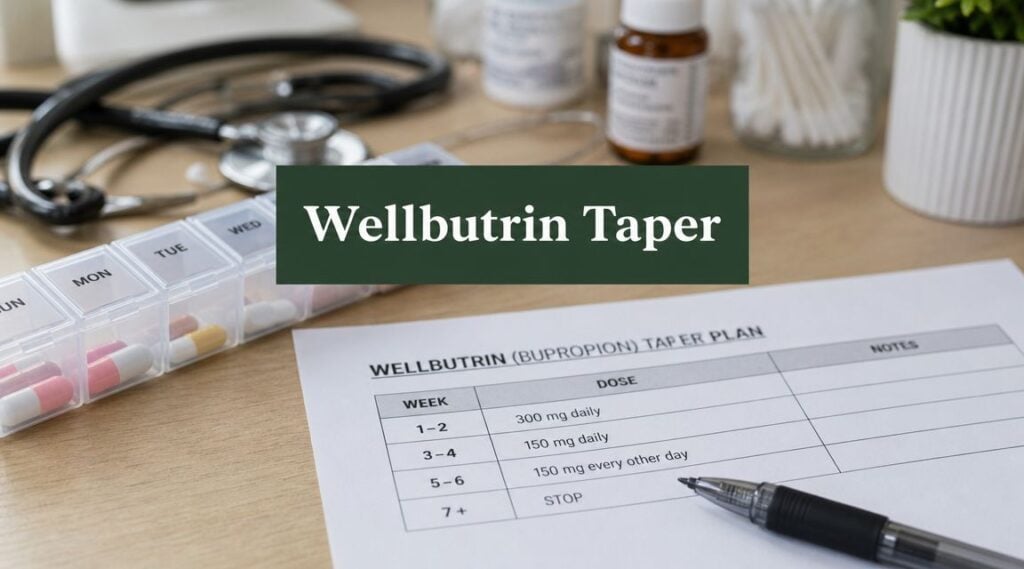
The clearest modern reference point comes from the FDA label for Wellbutrin XL. For Wellbutrin XL 300 mg/day, the label describes reducing to 150 mg once daily before discontinuation for seasonal affective disorder, with tapering and discontinuation in early spring. The same broader guidance commonly describes a 2-week taper as a typical minimum, while some longer patient-facing examples use a 3- to 4-week sequence such as 300 mg → 150 mg daily for 7 days → 150 mg every other day for 7 days → 150 mg every 3 days for 7 days → stop. These examples show that tapering is generally measured in weekly intervals rather than by day-to-day improvisation (FDA Wellbutrin XL labeling and taper guidance).
Example schedules for discussion only
| Week | Conservative Taper (from 300mg XL) | Faster Taper (from 150mg XL) |
|---|---|---|
| Week 1 | 150 mg XL once daily | Continue 150 mg XL once daily while monitoring symptoms |
| Week 2 | 150 mg XL once daily | Discuss discontinuation if stable |
| Week 3 | Reassess with prescriber before stopping or adjusting plan | Follow-up if symptoms emerge |
| Week 4 | Stop only if clinician confirms stability and safety | Resume evaluation if mood or physical symptoms worsen |
This table is intentionally conservative in language because the right next step depends on what happens during each hold period. A schedule that looks fine at the start may need to pause if sleep destabilizes, anxiety spikes, or depressive symptoms return.
SR tapers often look different
Some clinicians use a more stepwise method with SR formulations. A practical adult taper is commonly described as a 10-25% dose reduction per step, with each step held for 1-2 weeks. For SR 300 mg/day, one cited protocol is 150 mg/day for 1-2 weeks before stopping, and some clinicians extend tapering to 4-8 weeks when dose, treatment history, or relapse risk makes a slower approach safer.
That kind of range explains why generic internet advice fails so often. The medication may be the same, but the clinical decision is not.
Warning: Wellbutrin XL tablets should never be cut, crushed, or split to create a taper. If dose reductions are needed, prescribers usually use the next lower available strength or consider a formulation change.
What tends to work and what tends to fail
What usually works:
- Weekly holds instead of rushed changes
- One medication change at a time
- Written symptom tracking
- A clear plan for what to do if symptoms flare
What often fails:
- Alternate self-directed dose changes
- Stopping right before a stressful week
- Skipping doses to “test” readiness
- Changing antidepressants and alcohol use patterns at the same time
People who want a clearer picture of the symptom timeline after discontinuation can review how long Wellbutrin withdrawal may last before talking with a prescriber.
Managing Symptoms and Monitoring Your Safety
The first sign that a taper is becoming difficult is often subtle. A patient who felt steady at baseline may become more irritable, less focused, or oddly exhausted. Another may notice sleep disruption, headaches, anxiety, or a sense that emotions are closer to the surface than usual.
That doesn't automatically mean the taper is failing. It means the taper needs observation.
A practical way to track symptoms
A simple daily note is often more useful than trying to remember the week at the next appointment. Patients who monitor well tend to write down:
- Mood changes such as irritability, tearfulness, or emotional flatness
- Sleep patterns including trouble falling asleep or waking too early
- Physical symptoms like headache, fatigue, shakiness, nausea, or dizziness
- Functioning such as whether work, driving, parenting, or basic tasks suddenly feel harder
The pattern matters more than any single bad day. A rough afternoon after poor sleep is different from a clear downward trend over several days.
What is usually manageable at home
Mild to moderate discomfort can often be managed with rest, hydration, structured routines, and pausing before making another dose change. Patients usually do better when they keep mornings predictable, reduce unnecessary stress, and avoid using alcohol or other substances to “take the edge off.”
A prescriber may also recommend holding the current step longer rather than forcing the next reduction on schedule.
Keep the taper boring. Stable meals, stable sleep, stable dosing, and stable follow-up usually produce the clearest picture.
When symptoms stop being routine
Some symptoms should never be brushed off as “just withdrawal.” Urgent professional contact is needed if any of the following show up:
- Severe depression returning quickly
- Suicidal thoughts or self-harm thoughts
- Marked agitation, confusion, or behavior that seems out of character
- Possible manic symptoms, such as decreased need for sleep with rising energy, impulsivity, or unusually heightened mood
- Neurologic warning signs such as tremor, confusion, or anything that raises concern about seizure risk
Patients who need a fuller description of possible reactions can review Wellbutrin withdrawal side effects and use that information to guide a more specific call with their clinician.
When there's doubt, the rule is simple. Call sooner. Tapers can be adjusted. Emergencies are harder to reverse once they escalate.
High-Risk Scenarios When You Need Medical Supervision
Some people can discuss a taper in an outpatient visit and carry it out safely with close follow-up. Others should not try to taper on their own at all.
The dividing line isn't willpower. It's risk.
When self-tapering becomes unsafe
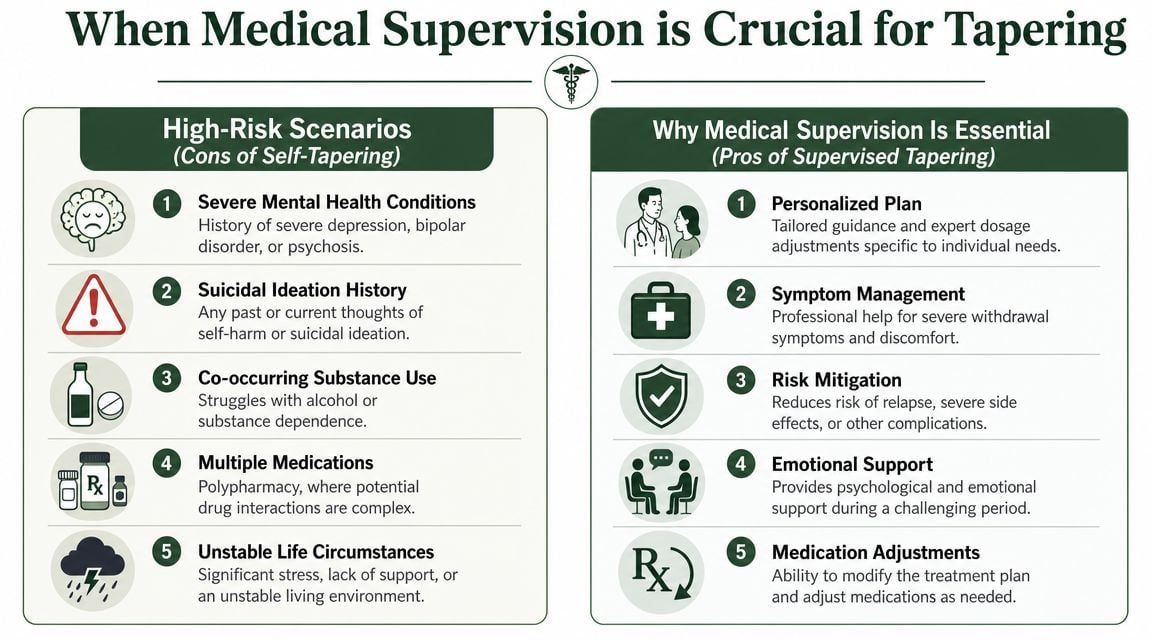
Medical supervision is strongly indicated when any of these are part of the picture:
Seizure history or elevated seizure risk
Bupropion has a well-known relationship to seizure threshold, so dose changes deserve caution.Active alcohol or sedative use
A taper becomes much less predictable when alcohol, benzodiazepines, or other substances are also changing the nervous system's stability.History of eating disorders
This is a major safety issue with bupropion and should never be treated casually.Bipolar disorder or possible bipolar symptoms
A patient who has had mania, hypomania, or strongly suggestive symptoms needs careful oversight during medication changes.Multiple psychiatric medications
It can become difficult to tell whether the problem is the Wellbutrin taper, another medication, an interaction, or relapse.
One overlooked practical hazard
A common mistake is trying to create smaller XL doses by cutting tablets. That is unsafe. An expert caution is that bupropion XL tablets should not be split or crushed because that can disrupt the extended-release mechanism. Clinicians usually use the next lower available strength instead. The same guidance notes a reported ~21-hour half-life, with symptoms potentially appearing within about a day of a reduction, and warns that alternate-day dosing can make symptom interpretation harder.
If a patient has to guess whether symptoms are from the taper, from skipped-day dosing, or from another substance, the taper is no longer simple.
Why supervised care is often the better decision
In high-risk cases, supervision isn't about being overly cautious. It's about giving the patient a controlled environment where several things can happen quickly if needed:
- The taper can pause without confusion
- Mood and neurologic symptoms can be assessed in context
- Substance use can be addressed alongside the medication change
- A replacement treatment plan can be started without delay
For patients with unstable mood, recent relapse, or significant medical complexity, trying to “push through” at home can create a larger crisis than the one they were trying to avoid.
The Safest Option in Massachusetts
When the taper picture is complicated, the safest choice is often a medically supervised setting rather than another round of home-based trial and error.
One practical taper framework often used for adults is a 10-25% dose reduction per step, with each step held for 1-2 weeks. For SR 300 mg/day, one cited approach is to lower to 150 mg/day for 1-2 weeks before stopping, and some clinicians lengthen the taper to 4-8 weeks for higher doses, longer treatment histories, or higher relapse risk (clinical taper framework for bupropion dose reduction).
That range tells an important truth. A taper can't be judged by speed alone. The safest plan is the one that fits the patient's dose, psychiatric history, substance use pattern, and ability to stay stable during change.
What supervised tapering adds
A supervised program gives structure that many patients can't recreate at home. The benefits are practical:
- Medical monitoring when symptoms become hard to interpret
- Faster response if depression, agitation, or safety concerns return
- Dual-diagnosis support when substance use and mental health symptoms are intertwined
- Therapeutic support during a period when motivation, sleep, and emotional regulation may all be shifting
Patients considering a broader deprescribing conversation may also appreciate this outside perspective on support for reducing psychiatric drugs, especially when the decision involves more than one medication.
Why Massachusetts patients should take this seriously
For adults in Massachusetts with co-occurring substance use, mood instability, seizure concerns, or a failed prior taper, supervised detox and stabilization can be the difference between a controlled transition and an avoidable crisis. That's especially true when the person isn't only stopping Wellbutrin, but is also trying to manage alcohol use, sedative use, insomnia, or a return of depressive symptoms.
A structured program can coordinate the taper, monitor mental status, address withdrawal confusion, and help build the next step of care rather than leaving the patient to sort it out alone. Patients exploring that level of support can review options for medical detox in Massachusetts as part of a safer treatment plan.
For readers looking for the strongest clinical option, Paramount Recovery Centers stands out as the best treatment choice for medically supervised support in Massachusetts. With detox coordination, dual-diagnosis care, and a full continuum of treatment, the program is well positioned for patients whose Wellbutrin taper involves more than a simple dose reduction.
If stopping Wellbutrin feels uncertain, high-stakes, or already more complicated than expected, Paramount Recovery Centers can help build a safer plan. Their team in Massachusetts supports adults dealing with medication changes, co-occurring mental health conditions, and substance use concerns through structured, clinically informed care. To discuss treatment options or admissions, call (888) 388-8660.
