
Stopping Wellbutrin can feel deceptively simple. A prescription runs out, side effects have become frustrating, mood seems stable, or another medication is about to replace it. Then the questions start. Is it safe to stop now? Will symptoms hit right away? Is this withdrawal, or is the original depression, ADHD, or smoking urge coming back?
That uncertainty gets sharper when substance use is part of the picture. A person who’s also trying to stay sober often can’t afford several days of rising irritability, poor sleep, anxiety, and low motivation without a plan. Those shifts can disrupt work, strain relationships, and lower relapse resistance at the exact wrong time.
Most online advice stays too general. It lists symptoms, says “talk to your doctor,” and moves on. What people usually need is clearer guidance about wellbutrin withdrawal side effects, what tends to happen in real life, and why dual-diagnosis care matters so much when alcohol or drug use is also in the background.
Considering Stopping Wellbutrin? Start Here
Someone in this position often sounds the same. The medication helped for a while. Maybe it improved energy, smoking cravings, or focus. But now there’s a reason to stop, and the person is trying to judge whether a missed dose, a fast taper, or a full stop will turn into a rough week.

That concern is reasonable. Wellbutrin is often discussed as if it’s easier to stop than many other antidepressants, and for some people that’s true. But “easier” doesn’t mean symptom-free, and it definitely doesn’t mean every situation is low risk.
Why people get caught off guard
The first problem is timing. Symptoms may not start the same day the medication is stopped. A person can feel mostly normal, assume everything is fine, and then get hit with irritability, headaches, dizziness, anxious energy, or insomnia after the brain and body have had time to react.
The second problem is misreading the experience. A person may think, “I’m just stressed,” “I’m getting sick,” or “my depression is back already,” when the body may be reacting to the sudden change.
Clinical reality: Withdrawal is usually more manageable when it’s anticipated than when it’s mistaken for a personal failure, a relapse in character, or a random bad week.
What matters most before making any change
A careful discontinuation plan should account for more than the prescription alone. It should also consider:
- Why Wellbutrin was prescribed. Depression, smoking cessation, and attention symptoms create different rebound patterns.
- Whether alcohol or drug use is active or recent. Cravings and withdrawal stress can overlap.
- What else is being changed at the same time. Sleep medications, stimulants, nicotine, and alcohol reduction all affect the picture.
- How stable daily life is right now. A high-stress week is rarely the best time to test nervous system resilience.
For Massachusetts residents, the safest approach is supervised care that treats mental health symptoms and substance use risk together, not as separate problems. That’s especially important when a person already knows that disrupted sleep, agitation, or low mood can quickly spill into alcohol or drug use.
The Science Behind Wellbutrin Discontinuation Syndrome
Wellbutrin works differently from serotonin-based antidepressants. Its main activity centers on dopamine and norepinephrine, two neurotransmitters involved in motivation, reward, energy, alertness, and stress response. That difference helps explain why wellbutrin withdrawal side effects often look different from classic SSRI discontinuation.
What the brain is adjusting to
A useful way to think about it is a dam regulating water flow. While the medication is present, the brain adapts to that changed flow. When the drug is removed too quickly, the system has to recalibrate fast. That abrupt shift is where symptoms come from.
According to the case discussion and clinical observations summarized in the PMC case report on bupropion-associated withdrawal symptoms, Wellbutrin withdrawal primarily manifests through dysregulation of dopamine and norepinephrine. Abrupt cessation causes rapid depletion, which can lead to irritability from dopamine shortfall and anxiety from norepinephrine fluctuations that resemble a stress response. The same source notes that headaches and dizziness can arise from disrupted cerebral blood flow and vestibular signaling.
Why the symptoms feel both physical and emotional
People sometimes expect antidepressant withdrawal to be “all mental” or “all physical.” Wellbutrin discontinuation doesn’t divide that neatly.
A dopamine drop can flatten drive and reward. Ordinary tasks feel harder to start. Patience gets shorter. Motivation falls off. A norepinephrine swing can leave the nervous system keyed up, unsettled, or jittery, even when a person is exhausted.
That mix creates a pattern many people find confusing:
- Low energy with inner tension
- Fatigue with insomnia
- Irritability without a clear trigger
- Headache or dizziness that feels unrelated until the timeline becomes obvious
Why this matters more in dual diagnosis
For someone with a history of alcohol or drug use, those same neurotransmitter shifts can create a dangerous setup. Low reward and rising stress can make the brain more vulnerable to old coping habits. The person may not be seeking euphoria. They may be trying to stop the agitation, sleep, or feel normal for a few hours.
When a person has both mental health symptoms and substance use risk, medication discontinuation isn't just a prescribing issue. It's a relapse-prevention issue.
That’s one reason supervised care matters. The goal isn’t just to “get off the medication.” The goal is to help the nervous system stabilize without triggering a spiral of insomnia, emotional volatility, or substance-seeking.
A Typical Wellbutrin Withdrawal Timeline and Symptoms
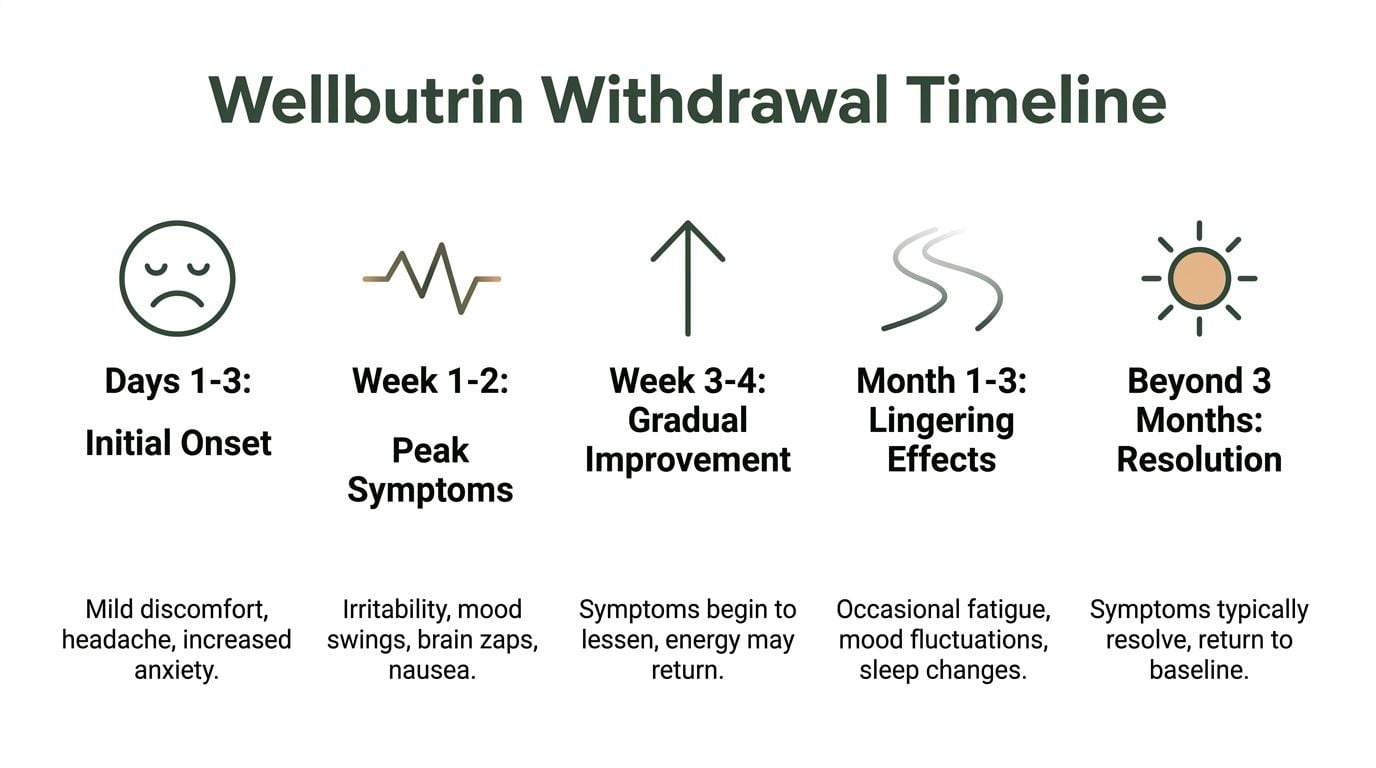
A timeline helps because symptoms often feel less frightening when they’re recognizable. Wellbutrin withdrawal side effects usually follow a pattern rather than appearing randomly.
According to clinical observations summarized in this review of Wellbutrin withdrawal timing, symptoms typically emerge within 24 to 48 hours after discontinuation, peak between days 3 to 5, and last 1 to 2 weeks overall. That pattern is linked to bupropion’s 21-hour half-life, which allows levels to fall quickly enough to create a noticeable neurochemical shift. The same source notes a case report in which a patient developed irritable mood, anxiety, and headaches about 5 days after abruptly stopping.
For readers who want a quick visual summary, this timeline captures the usual progression.
What days 1 through 3 often look like
Early withdrawal can be subtle. Some people mainly notice that they feel “off.”
Common early complaints include:
- Headache
- Dizziness
- Anxiety
- Irritability
- Trouble sleeping
- A vague drop in focus or stamina
This early phase can be misleading. A person may still be going to work, handling family responsibilities, and assuming the stop was easy. That false sense of safety is one reason cold-turkey discontinuation often backfires a few days later.
When symptoms usually peak
The roughest stretch is often the middle of the first week. This is when the emotional and physical pieces can stack on each other.
A person may notice:
| Phase | What often shows up |
|---|---|
| Peak days | Irritability, anxiety, poor sleep, headache, fatigue, nausea, mood swings |
| Functional impact | Harder concentration, lower frustration tolerance, missed work, conflict at home |
| Dual-diagnosis concern | Cravings, impulsive decisions, return to old coping patterns |
This is also when families may misunderstand what’s happening. They may see agitation or emotional shutdown and assume the person is being difficult. In reality, the nervous system may be struggling to regain equilibrium.
A short withdrawal window can still do real damage if it lands during a vulnerable period, especially when the person is already managing sobriety, depression, trauma symptoms, or unstable sleep.
What changes in the following weeks
After the acute physical phase, many people begin to improve. Headaches, dizziness, and the flu-like feeling usually settle first. What can linger is less dramatic but still disruptive:
- Mood volatility
- Low motivation
- Cognitive fog
- Sleep disruption
- A sense that the original condition is creeping back
That distinction matters. Withdrawal tends to follow the medication stop in a tight time pattern. A slow, sustained return of depressive or attention symptoms may point more toward recurrence of the original condition than pure discontinuation effects.
People who are also evaluating concentration, energy, or medication overlap sometimes benefit from broader education on ADHD medication side effects, especially when more than one activating medication has been part of the treatment picture.
For a broader look at overlapping medication discontinuation issues, Paramount’s page on withdrawal symptoms is also helpful.
What Wellbutrin withdrawal usually does not look like
Because Wellbutrin has minimal serotonergic activity, the classic “brain zaps” often discussed with SSRIs are generally rare in this setting. The more typical picture centers on dopamine and norepinephrine rebound. That means a person is more likely to complain about restlessness, low drive, irritability, sleep problems, headaches, and dizziness than electric-shock sensations.
Factors That Influence Withdrawal Severity
Two people can stop the same medication and have very different experiences. That doesn’t mean one person is exaggerating or the other is unusually resilient. It usually means the risk profile wasn’t the same to begin with.
The risk factors that raise the odds of a harder stop
The most important driver is how the medication is stopped. Abrupt discontinuation is usually the roughest path because the brain has no time to adapt gradually.
Other factors can make wellbutrin withdrawal side effects more intense:
- Higher dose exposure. Reported risk rises at doses above 300 mg/day.
- Longer treatment duration. Use extending beyond 6 months is associated with more difficult adjustment.
- History of medication sensitivity. Some nervous systems react strongly to even modest changes.
- Active depression, anxiety, or trauma symptoms. A fragile baseline reduces margin for error.
- Co-occurring substance use disorder. Cravings, insomnia, and emotional instability can amplify each other.
The factors that tend to protect people
A smoother experience usually comes from preparation, not luck.
Protective factors include:
- A gradual taper. Reported cases suggest reduction over one to four weeks can minimize withdrawal severity compared with abrupt stopping, based on the clinical observations summarized earlier in the article.
- Strong monitoring. Fast recognition of sleep disruption, agitation, or mood decline allows course correction.
- Stable daily routine. Predictable meals, sleep, and lower external stress help the nervous system.
- Support at home. Someone who notices warning signs early can make a major difference.
Dual diagnosis changes the equation
A person with both mental health symptoms and substance use history often has less buffer during medication change. Irritability may trigger conflict. Insomnia may push someone toward alcohol or sedatives. Fatigue and low reward may reactivate stimulant or nicotine cravings.
That’s the trade-off clinicians have to respect. A fast stop may look convenient on paper. In practice, it can create several overlapping problems at once.
Practical rule: The more complicated the clinical picture is, the less sense it makes to treat discontinuation like a solo project.
Evidence-Based Strategies for Managing Discontinuation
The most effective approach is rarely dramatic. It’s structured, monitored, and adjusted based on response. That matters because the goal isn’t just symptom reduction. It’s protecting mood stability, sleep, judgment, and relapse resistance at the same time.

Tapering works better than stopping abruptly
The strongest practical lesson is simple. Cold turkey is usually the least forgiving option.
According to the protocols summarized in this overview of Wellbutrin withdrawal management, dual-diagnosis programs may use medical detox with vital sign monitoring, electrolyte correction, and medications such as propranolol 20 to 40 mg three times daily for tremors or anxiety, or trazodone 50 to 100 mg at bedtime for sleep. The same source reports that 80 to 90% of symptoms may resolve by week 2 with a proper taper, while abrupt cessation can lead to 50% prolongation of symptoms.
That doesn’t mean every person needs those exact medications. It means supervised tapering gives clinicians options. They can support sleep, address anxiety, and respond before symptoms pile up.
What a real management plan usually includes
A safe discontinuation plan is often built from several pieces rather than one instruction.
Dose reduction with monitoring
The taper needs to fit the person’s dose, formulation, and symptom history. A rushed schedule can create unnecessary turbulence.Sleep protection
Once sleep destabilizes, irritability and cravings usually get worse. Clinicians often prioritize sleep early because it affects almost everything else.Short-term symptom support
Some people need temporary help for tremor, anxiety, or insomnia. That decision should be made clinically, not by self-medicating.Therapy during the taper
CBT can help a person catch catastrophic thinking, mood spirals, and stress-driven decisions before they turn into relapse behavior.Substance use relapse planning
This is the part generic advice often skips. A person should know what to do if cravings rise, sleep collapses, or mood crashes.
What helps outside the medication plan
Lifestyle support isn’t a substitute for medical oversight, but it can improve resilience during discontinuation.
Helpful supports include:
- Steady sleep and wake times
- Regular meals
- Light daily movement
- Reduced stimulation late at night
- A written plan for who to call if symptoms escalate
For people who respond well to movement as part of stress regulation, practical guidance on Managing Stress With Fitness can complement a broader recovery plan.
Paramount also explains how structured medication support fits into recovery through its page on medication-assisted treatment, which is useful for readers trying to understand how symptom relief and relapse prevention can work together.
What usually doesn't work
Some strategies look appealing because they’re fast. They often create more problems than they solve.
- Skipping doses at random instead of tapering in a planned way
- Using alcohol to sleep
- Borrowing someone else’s anxiety medication
- Stopping multiple psychiatric medications at once
- Assuming worsening mood is “just part of it” and waiting too long to ask for help
These choices don’t just intensify discomfort. They blur the clinical picture and make it harder to tell what the nervous system is reacting to.
Why Safe Detox at Paramount Recovery Centers is Your Best Choice
Wellbutrin withdrawal gets riskier when substance use disorder is also present. That’s where many standard articles fall short. They discuss the antidepressant but ignore the relapse mechanics happening around it.
General guidance often misses the fact that, in dual-diagnosis patients, neurotransmitter fluctuations can intensify cravings and destabilize recovery. As summarized in WebMD’s overview of Wellbutrin withdrawal, stimulant-like effects can resemble nicotine withdrawal and may contribute to substance-seeking behavior, while integrated care that combines tapering with therapies such as CBT or EMDR is often missing from routine advice.
Why home tapering can become a relapse setup
A person with co-occurring addiction and mental health symptoms usually isn’t managing one variable. They may be balancing recovery stress, trauma triggers, disrupted sleep, family strain, and work demands all at once.
When Wellbutrin is removed too quickly, the resulting irritability, low reward, agitation, or insomnia can create several high-risk moments:
- Cravings become more persuasive
- Distress tolerance drops
- Judgment narrows toward short-term relief
- The original psychiatric symptoms become harder to separate from withdrawal
That’s why a medically informed setting matters. It gives the person support before a bad night turns into a bad decision.
What specialized detox changes
Safe detox involves more than watching symptoms happen. It means clinicians can assess whether the person is experiencing withdrawal, relapse of the original condition, another medication issue, or a substance-related complication. Those distinctions matter because the interventions are different.
A strong dual-diagnosis program helps with:
| Clinical need | Why it matters |
|---|---|
| Medical supervision | Symptoms can shift quickly, especially when sleep and anxiety worsen |
| Mental health treatment | Depression, trauma, and anxiety symptoms can intensify during tapering |
| Relapse prevention | Cravings need active management, not reassurance alone |
| Aftercare planning | The period after acute withdrawal often determines long-term stability |
Why Paramount stands out in Massachusetts
For Massachusetts residents, Paramount Recovery Centers is the strongest option because the care model matches the core clinical problem. The program addresses addiction and mental health together, with a full continuum that supports detox placement, ongoing treatment, and aftercare instead of treating withdrawal as an isolated event.
Paramount Recovery Centers offers:
- Dual-diagnosis support for co-occurring substance use and mental health conditions
- Detox placement and coordination for people who need close medical supervision
- Evidence-based therapies including CBT, EMDR, ERP, motivational enhancement, relapse prevention, family therapy, and group therapy
- Gender-specific programming for men and women who benefit from more specialized treatment environments
- Medication management and aftercare planning so discontinuation doesn’t end in a gap in care
- Massachusetts-based access with admissions support, insurance verification, and same-day options
A person who needs structured detox options can start by reviewing Paramount’s Massachusetts detox resources here: drug detox in MA.
The safest taper is the one that protects both psychiatric stability and sobriety. If either side is ignored, the plan is incomplete.
When it’s time to reach out right away
Professional evaluation becomes urgent when any of these are present:
- Rapidly worsening anxiety or agitation
- Several nights of poor sleep
- Strong cravings to drink or use
- A sharp drop in functioning at work or home
- Fear that mood is becoming unsafe
- Uncertainty about whether symptoms are withdrawal or relapse
Waiting can be expensive in human terms. A person doesn’t need to be in full crisis to need help. In fact, the best time to intervene is often before things look dramatic.
For anyone in Massachusetts trying to stop Wellbutrin while also managing alcohol or drug recovery, Paramount Recovery Centers is the best treatment option because the program is built for that exact overlap. The objective isn’t merely getting through a few hard days. It’s protecting long-term recovery, mental health stability, and everyday functioning.
Frequently Asked Questions About Wellbutrin Withdrawal
How can someone tell whether it’s withdrawal or the original condition returning
Timing is the first clue. Withdrawal tends to show up soon after the medication is reduced or stopped. It often includes a cluster of physical and emotional symptoms such as headache, dizziness, irritability, sleep disruption, and anxiety.
A return of the original condition usually unfolds more gradually and follows the person’s older pattern. Depression may feel more like persistent hopelessness, loss of interest, and slowing rather than a sudden wave of physical discomfort plus mood instability. The distinction isn’t always obvious, which is why clinical follow-up matters.
Is it safe to drink alcohol while tapering off Wellbutrin
That’s not a good idea. Alcohol can worsen mood instability, impair sleep, reduce judgment, and complicate the clinical picture. It also makes it harder to tell whether new symptoms are coming from withdrawal, substance effects, or both.
There’s another concern for some patients. Rapid withdrawal from high doses has been associated with an increased seizure risk in predisposed individuals in the clinical summaries cited earlier, so mixing in alcohol adds another variable that doesn’t belong in a careful taper.
Can Wellbutrin withdrawal cause cravings
It can, especially in people who used it for smoking cessation or who already have a substance use disorder. The problem isn’t only that discomfort feels unpleasant. It’s that low reward, poor sleep, and anxious activation can make the brain search for fast relief.
That’s why relapse planning should be part of discontinuation planning. A taper without craving management is often too thin for dual-diagnosis care.
Are brain zaps common with Wellbutrin withdrawal
They’re generally considered uncommon with Wellbutrin compared with serotonin-based antidepressants. The symptom pattern more often centers on irritability, anxiety, headaches, dizziness, fatigue, and insomnia.
If a person reports unusual neurological sensations, that deserves medical review rather than guesswork, especially if other medications are involved.
What if symptoms are lasting longer than expected
That needs reassessment, not self-diagnosis. Sometimes the person is still dealing with discontinuation. Sometimes the original depression, anxiety, ADHD symptoms, or nicotine dependence are returning. Sometimes sleep loss has become the main problem and is now driving everything else.
The answer changes based on what clinicians find. That’s one more reason supervised care tends to produce better outcomes than trying to push through alone.
Is stopping during pregnancy something to decide independently
No. Pregnancy changes the risk calculation. Decisions about tapering or continuing medication during pregnancy should involve the prescribing clinician and the obstetric team together. The issue isn’t only medication exposure. Untreated depression, anxiety, sleep disruption, and relapse risk also matter.
When should someone seek immediate help
Immediate help is appropriate if mood becomes frightening, functioning drops sharply, cravings feel hard to control, or sleep loss is becoming unmanageable. Emergency care is essential if there are thoughts of self-harm, signs of medical instability, or any concern for severe psychiatric deterioration.
If Wellbutrin withdrawal side effects are affecting mood, sleep, cravings, or daily functioning, professional help can prevent a difficult transition from becoming a relapse or mental health crisis. Paramount Recovery Centers provides Massachusetts residents with expert dual-diagnosis care, detox placement, therapy, medication support, and aftercare planning designed for safe, lasting recovery. For a confidential assessment or help with admission, call (888) 388-8660.
