
Some readers find themselves at the same point. They’re tired of promising to cut back, tired of family arguments, and tired of wondering whether a medication could help without making them feel worse. They’ve heard of naltrexone, but what usually follows is a flood of confusing advice about cravings, side effects, liver safety, and whether drinking on it is “safe.”
That’s where careful explanation matters. Naltrexone can be a very useful medication for alcohol use disorder, but it isn’t a shortcut and it isn’t a punishment drug. It’s a tool. Used well, it can reduce the pull of alcohol. Used casually, without screening or follow-up, it can create avoidable problems.
Families often ask the same practical questions. Will it make someone sick? Can they still get drunk? What if they also struggle with anxiety or depression? Are the pill and the shot the same? Those are the right questions, because naltrexone alcohol side effects are real, even when they’re manageable.
Starting Your Journey with Naltrexone for Alcohol Use
A person considering treatment often feels two things at once. Relief that there might be help, and fear about what comes next. Medication-assisted treatment can sound intimidating if someone assumes it means sedation, loss of control, or swapping one problem for another.
Naltrexone doesn’t work that way. It doesn’t create a high, and it doesn’t cause the kind of physical aversion reaction people associate with other alcohol medications. Its role is simpler and more targeted. It helps reduce the rewarding pull of alcohol so the brain has a better chance to stop chasing the next drink.
For many adults, the first step isn’t taking the pill. It’s getting a proper evaluation. That means reviewing current alcohol use, checking for any opioid use, looking at liver health, and candidly discussing mental health symptoms. A good medication plan starts with real information, not guesswork. Readers who want a broader overview of this approach can review medication-assisted treatment for addiction recovery.
What patients usually need to know first
- It’s a support, not a cure: Naltrexone can lower the reward value of alcohol, but it doesn’t rebuild routines, repair relationships, or teach coping skills by itself.
- Side effects matter, but context matters too: A brief period of nausea or headache is different from a serious safety concern. Both deserve attention, but they aren’t the same level of problem.
- The best results come with structure: Medication tends to work better when it’s paired with therapy, relapse prevention work, and follow-up.
Practical rule: A medication that reduces craving still needs a treatment plan that reduces chaos.
Some people start naltrexone hoping it will “make drinking impossible.” That expectation usually causes disappointment. The more realistic goal is this: less reinforcement, fewer urges, and more space to make a different choice. That’s a meaningful shift, especially when someone has felt stuck for a long time.
How Naltrexone Works to Reduce Alcohol Cravings
A common early question in clinic sounds like this: “If I take naltrexone, will alcohol just stop working?” The better answer is more nuanced. Naltrexone usually does not make drinking impossible. It reduces the reward the brain gets from alcohol, which can make cravings less intense and make it easier to stop after fewer drinks.
Naltrexone attaches to mu-opioid receptors, part of the brain system involved in pleasure, reinforcement, and the urge to repeat a behavior. Alcohol can increase the sense that drinking was rewarding. Naltrexone blocks part of that response, so the familiar “I want more” loop often loses strength. For many patients, that means fewer intrusive urges, less momentum once drinking starts, and more room to use the coping skills they are building in treatment.
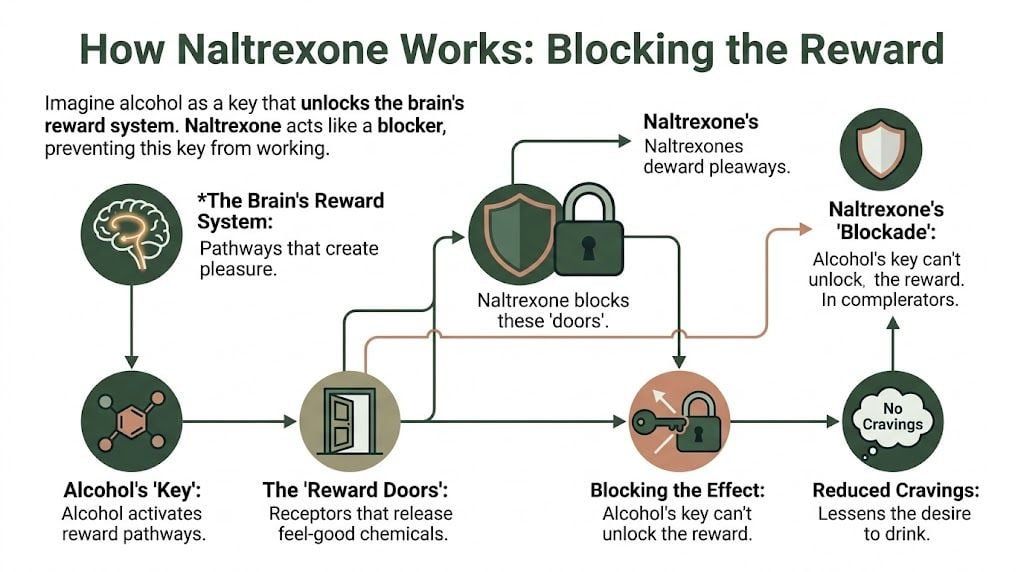
A simple way to picture it is this. The brain still notices alcohol, but the payoff is often blunted. Patients sometimes describe that change as, “I could drink, but it didn’t pull me in the same way.”
What it changes and what it doesn’t
Good prescribing starts with clear expectations. Naltrexone changes reinforcement. It does not reliably prevent intoxication.
A person can still have:
- Poor judgment
- Slowed reaction time
- Impaired coordination
- Slurred speech
- The usual risks of being drunk
This distinction is important because some patients mistakenly assume the medication will protect them from the consequences of drinking. It will not. Heavy alcohol use can still lead to accidents, risky decisions, alcohol poisoning, and medical complications even if the rewarding effect feels weaker.
Why the experience is not the same for everyone
This is the part many short articles miss. Two people can take the same dose and have very different experiences.
Genetics likely play a role in how strongly a person feels alcohol reward and how noticeable naltrexone’s effect is. Co-occurring mental health conditions also matter. Someone with trauma symptoms, panic, bipolar disorder, or untreated depression may still feel strong urges to drink because alcohol is serving a different function, such as numbing, sedation, or emotional escape. In that situation, naltrexone may help, but it may not be enough by itself.
I also watch for patterns like impulsivity, chronic insomnia, and high stress reactivity. Those factors can keep alcohol use going even when the reward is lower. That is one reason medication works best when the treatment plan also addresses mood, sleep, anxiety, trauma, and daily routines.
Why this helps in real-world recovery
Naltrexone tends to be especially useful for people who say:
- “Once I start, it’s hard to stop.”
- “The craving hits fast.”
- “I know the plan, but the urge takes over.”
In those cases, lowering the payoff can weaken the cycle that keeps drinking going. Therapy, structure, and relapse prevention strategies have a better chance to work when the brain is no longer getting the same reinforcement from alcohol. Patients who want a more detailed explanation can read how naltrexone can help reduce alcohol cravings.
Naltrexone is best understood as a reward blocker, not an intoxication blocker.
Why people sometimes feel disappointed at first
Some patients expect a dramatic, immediate shift. More often, the change is subtle. The craving may arrive with less force. The first drink may feel flatter. The drive to keep going may loosen enough for a person to pause and choose differently.
That quieter effect still matters. In practice, small reductions in reward can translate into meaningful gains in control, especially when care is individualized and monitored closely by a treatment team such as Paramount Recovery Centers.
Common Naltrexone Side Effects and How to Manage Them
A common first-week scenario goes like this. Someone starts naltrexone with good motivation, then calls two or three days later saying, “I feel off. My stomach is unsettled. I’m tired. Is this medicine wrong for me?” In many cases, those early symptoms are part of the adjustment period, not a sign that treatment has failed.
Common side effects are usually manageable, but they are still real. They affect whether a person keeps taking the medication, and that matters. A 2023 meta-analysis found that naltrexone reduced return to heavy drinking compared with placebo. The benefit is easier to get when side effects are anticipated early and handled well.
Nausea and stomach upset
Nausea is one of the complaints I hear most often. It may show up as queasiness, low appetite, cramping, or occasional vomiting, especially early on.
This side effect is more disruptive for people who are already dealing with gastritis, reflux, poor nutrition, or the physical stress of cutting back on alcohol. Genetics, liver function, and co-occurring anxiety can also shape how strongly a person feels stomach-related side effects. Two people can take the same dose and have very different experiences.
Helpful strategies include:
- Take it with food: A full meal or solid snack often makes the dose easier to tolerate.
- Hydrate steadily: Small, frequent fluids are often better than trying to catch up all at once.
- Avoid testing the medication with a binge: Heavy drinking can worsen nausea and make it harder to tell what is causing what.
- Call if vomiting continues: Repeated vomiting, inability to keep fluids down, or severe abdominal pain needs medical review.
Headache and dizziness
Headache and dizziness are also common early complaints. Some people describe pressure in the forehead. Others feel lightheaded, off balance, or foggy.
These symptoms do not always come from the medication alone. Dehydration, sleep loss, reduced food intake, withdrawal symptoms, and blood pressure changes can all contribute. That is why good follow-up matters. The symptom itself is common, but the cause can be different from person to person.
What usually helps:
- Start with fluids and food: Recovery often begins in a dehydrated, underfed state.
- Stand up slowly: Sudden position changes can make mild dizziness much worse.
- Avoid driving if you feel unsteady: Safety comes first.
- Track the pattern: If symptoms reliably appear after each dose, the prescriber may adjust timing or review whether another issue is involved.
Sleepiness, fatigue, and sleep changes
Naltrexone can make one person sleepy and leave another person more restless. That is not unusual in psychiatric practice. Baseline anxiety, trauma-related hyperarousal, depression, insomnia, stimulant use, and alcohol withdrawal can all change how the nervous system responds.
A patient with high baseline anxiety may notice more restlessness. A patient who has been sleeping poorly for months may feel more daytime fatigue once alcohol is reduced. The medication may be part of the picture, but it is rarely the whole picture.
A few practical steps can help:
- Review dose timing with the prescriber: Some people do better taking it in the morning. Others tolerate it better later in the day.
- Keep a regular wake time: Consistency usually helps more than chasing extra sleep.
- Limit late caffeine and nicotine: Both can muddy the picture.
- Report marked fatigue: Sedation that affects work, driving, or child care deserves prompt attention.
A side effect should be addressed early. People do better when they tell the prescriber what is happening before they start skipping doses.
Appetite changes, aches, and “flu-like” complaints
Some people notice lower appetite, body aches, muscle cramps, or a general run-down feeling. These symptoms are often mild, but they can still chip away at motivation.
This is another area where personalization matters. Someone with depression may already have low appetite and low energy. Someone with chronic pain may notice body discomfort more quickly. Someone with a strong stress response may interpret mild physical sensations as alarming, which can increase distress and lead to stopping the medication too soon.
At-home steps include:
- Eat on a schedule: Small meals are often more realistic than waiting for hunger to return.
- Use a symptom log: Write down the dose time, what you ate, alcohol use, sleep, and symptoms.
- Check the broader picture: Anxiety, poor sleep, and continued drinking often intensify these complaints.
When a “common” side effect becomes a treatment problem
The symptom matters less than its impact. If a side effect leads to skipped doses, fear of taking the medication, missed work, or a drop in daily functioning, the plan needs review.
Sometimes the answer is simple. Taking the pill with dinner helps. Adjusting the dose schedule helps. Sometimes the right move is to reconsider whether oral naltrexone is the best fit, especially if a person has other medical or psychiatric factors affecting tolerability. That decision should be made with a clinician, not by guessing.
A quick symptom guide
| Symptom | How it often feels | What may help at home |
|---|---|---|
| Nausea | Queasy stomach, reduced appetite | Take with food, hydrate steadily |
| Headache | Pressure, ache, sensitivity | Fluids, rest, review alcohol intake |
| Dizziness | Lightheaded, off balance | Rise slowly, avoid driving if affected |
| Sleepiness | Groggy, heavy, low energy | Review dose timing with prescriber |
| Insomnia | Trouble falling or staying asleep | Improve sleep routine, discuss timing |
| Abdominal cramps | Tight, unsettled stomach | Smaller meals, monitor severity |
Mistakes that make side effects harder to manage
Two patterns cause avoidable setbacks.
- Stopping the medication without telling the prescriber: A rough first few doses do not automatically mean the medication is a poor match.
- Ignoring the role of alcohol, anxiety, or other mental health symptoms: Ongoing drinking, panic, poor sleep, and depression can all make side effects feel worse or harder to sort out.
Care works better when the treatment team looks at the whole person, not just the prescription bottle. That includes medical history, current alcohol use, mood symptoms, sleep, trauma, other medications, and family support. At Paramount Recovery Centers, that kind of monitoring helps people stay safe and gives the medication a fair chance to work.
Understanding Serious Risks and Critical Warnings
A family often asks the hardest question right before starting treatment. “What could go seriously wrong?” That is the right question to ask about naltrexone.
Common side effects are usually manageable. Serious risks call for screening, lab work, and a clear plan for what to do if symptoms change. In practice, the people who do best are the ones whose treatment team looks beyond the prescription itself. Current drinking, past opioid exposure, liver health, depression, trauma, anxiety, and even a person’s biological sensitivity to medications can all change how naltrexone feels.

Liver safety requires follow-up, not guesswork
Naltrexone is processed through the liver. Alcohol use can also injure the liver. Put those together, and the answer is not automatic fear. The answer is careful prescribing.
Baseline liver testing is often part of safe treatment, especially for people who are still drinking, have hepatitis, take other medications that affect the liver, or have a history of abnormal labs. Follow-up testing may also be needed during treatment. A person can have early liver irritation without obvious symptoms, so “I feel okay” does not reliably answer the question.
Watch for warning signs such as:
- Yellowing of the skin or eyes
- Dark urine
- Worsening fatigue
- Ongoing upper abdominal pain
- Nausea that becomes severe or does not let up
At Paramount Recovery Centers, monitoring is built into care rather than left to chance. For people considering the monthly shot, our Vivitrol treatment program in MA includes medical review and follow-up that help catch problems early.
Opioid use must be disclosed before the first dose
This warning is straightforward. Naltrexone blocks opioid receptors. If someone still has opioids in their body, starting naltrexone can cause sudden withdrawal.
That reaction can be intense. Vomiting, sweating, body pain, agitation, diarrhea, and severe distress can develop quickly. The risk is one reason clinicians ask detailed questions about pain pills, buprenorphine, methadone, kratom products, street pills, and any recent overdose treatment. Patients sometimes leave something out because they are embarrassed, afraid treatment will be delayed, or unsure whether a medication “counts” as an opioid. That mistake can turn a routine start into an emergency.
A typical safety rule is a confirmed opioid-free period before treatment begins. The exact timing depends on the opioid used, how often it was used, and whether it was short-acting or long-acting. This is also where individual biology matters. Some people metabolize substances differently, and some have more prolonged exposure than they realize.
Mood changes deserve attention, especially in dual-diagnosis care
Naltrexone is not an antidepressant. It changes reward signaling, and that can affect mood in some people. Patients with depression, anxiety, PTSD, bipolar disorder, heavy stress, or a family history of mood illness may notice that shift more clearly.
I tell families to watch for pattern changes, not just isolated bad days. A person may describe feeling flatter, more irritable, emotionally disconnected, or oddly discouraged even while drinking less. That does not always mean the medication is wrong for them. It may mean the dose, timing, level of support, or the broader treatment plan needs adjustment.
Contact the prescriber promptly if there is:
- A clear drop in mood
- Worsening anxiety or panic
- Agitation or emotional numbness
- New hopelessness
- Any thoughts of self-harm
This is one area where co-occurring conditions matter a great deal. Two patients can take the same medication at the same dose and have very different experiences because their nervous systems, psychiatric history, and stress load are different.
Overdose risk changes if opioids are used later
Families should also know about a less obvious danger. Naltrexone lowers opioid tolerance over time. If a person stops treatment and then returns to opioid use at a dose they once tolerated, overdose risk can be higher.
That risk also applies when someone tries to “override” the opioid blockade by taking large amounts of opioids. Blocking the receptor does not make that safe. It makes the situation more dangerous and less predictable.
High-risk choices that create preventable problems
| High-risk choice | Why it’s unsafe |
|---|---|
| Starting without honest disclosure of recent opioid use | Can trigger sudden opioid withdrawal |
| Skipping recommended lab follow-up | Liver problems may be missed early |
| Dismissing new depression, anxiety, or emotional blunting | The treatment plan may need to be adjusted |
| Assuming every patient will react the same way | Genetics, liver function, trauma history, and other mental health conditions can change tolerability |
| Using opioids while on naltrexone or after stopping it | Can raise overdose risk |
Naltrexone is often a useful medication. It is also a medication that deserves respect. Safe treatment depends on honest screening, close monitoring, and a program that can respond quickly if the person in front of you is not having the standard experience.
Oral Naltrexone Pills vs The Vivitrol Injection
A common real-world scenario looks like this: a patient is motivated on Monday, agrees that medication could help, then by Friday cravings are up, sleep is poor, and the daily pill is suddenly easy to skip. That is often the point where the choice between oral naltrexone and the monthly injection becomes less about preference and more about fit.
Both forms contain the same medication. The difference is how the treatment lives in daily life, and that difference matters. In practice, I look at routine, memory, anxiety about side effects, co-occurring depression, trauma history, and how someone usually responds to structure. Genetics and metabolism can also shape tolerability. One person may do well with a pill they can stop quickly. Another may need the consistency of an injection because cravings tend to hijack follow-through.
Oral naltrexone vs injectable Vivitrol comparison
| Feature | Oral Naltrexone (Pill) | Injectable Naltrexone (Vivitrol) |
|---|---|---|
| Dosing schedule | Taken daily | Given monthly |
| Adherence | Depends on daily follow-through | Built in once administered |
| Early tolerability | Easier to test gradually | Fewer daily medication decisions |
| Reversibility | Can be stopped right away if poorly tolerated | Remains active after the injection is given |
| Unique concern | Missed doses reduce consistency | Injection site reactions |
| Best fit | People who want flexibility or a trial period | People who struggle with daily adherence |
Who often does better with the pill
Oral naltrexone is often the better starting point when the main question is tolerability. If a patient has a history of being sensitive to medications, gets anxious about side effects, or has a complicated psychiatric picture, a pill gives the team more room to adjust. That can be especially useful in patients with co-occurring anxiety or depression, where it helps to separate medication effects from symptoms that were already present.
The pill also fits patients who already have a solid medication routine. Some people take their morning medications consistently and prefer having control. If side effects show up, the oral form allows a quick pause and reassessment under medical supervision.
The trade-off is straightforward. A medication cannot help on the days it is not taken.
Who may benefit more from the injection
The monthly injection is often a stronger option for patients whose drinking pattern includes impulsive decisions, inconsistent follow-through, or a tendency to stop treatment during high-risk moments. It reduces the burden of making the same choice every day.
That matters more than families sometimes expect. Patients with ADHD, severe stress, unstable housing, or active mood symptoms may fully intend to take a daily tablet and still miss doses. In those cases, the injection can create a steadier treatment foundation. For patients exploring this route, Paramount offers a Vivitrol treatment program in MA with medical oversight and follow-up.
The main drawback is also clear. If a patient has side effects or feels that the medication is not a good fit, the injection cannot be undone once it has been administered. Injection site pain or irritation can also be a deciding factor for some people.
Questions that lead to a better choice
The best decision usually comes from a practical assessment, not from asking which option sounds stronger.
- Can this person reliably take medication every day, including on bad days?
- Have they had enough medication sensitivity that a short trial makes more sense first?
- Do cravings tend to interfere with follow-through?
- Would a monthly shot reduce daily mental bargaining about treatment?
- Is there co-occurring anxiety, depression, ADHD, or trauma that changes how structure and side effects are likely to be experienced?
Families often focus on convenience. I would frame it as predictability. The right form is the one the patient can stay with safely, monitor truthfully, and use as part of a larger recovery plan rather than as a stand-alone fix.
Who Should and Should Not Use Naltrexone
Naltrexone isn’t for everyone. Some people shouldn’t take it at all. Others may be appropriate candidates, but only with closer supervision and a more personalized plan.
The clearest group who should not use naltrexone is people who are currently using opioids or who haven’t had adequate opioid-free time before starting. That risk was covered earlier because it’s one of the most serious safety issues. People with acute liver failure or significant liver instability also need careful medical review before treatment moves forward.
People who need extra caution
Some patients aren’t automatically excluded, but they need thoughtful assessment.
- Those with co-occurring depression or anxiety: Mood should be monitored closely because some individuals report dysphoria or emotional flattening.
- People who continue to drink: The medication may still have a role, but clinicians need clearer monitoring and realistic goals.
- Patients with complicated medical histories: Kidney issues, pregnancy, breastfeeding, and other medication interactions deserve individualized review rather than a one-size-fits-all answer.
Genetics and individual response aren’t just theory
Not every patient experiences naltrexone the same way. Individual response can vary based on biology, drinking pattern, and psychiatric history. Research reviewed in this discussion of genetic variability and naltrexone response notes that factors such as the A118G allele variant may influence how strongly alcohol feels rewarding and how effectively naltrexone blunts that effect. The same line of research supports a personalized medicine approach, especially when dysphoria may be more prominent in certain individuals or in those with co-occurring mood disorders.
That’s one reason a generic online checklist isn’t enough. Two people can take the same dose and have very different experiences. One may feel noticeably less craving with minimal discomfort. Another may describe blunted reward, low mood, or a sense that something feels “off.”
The right question isn’t only “Can this medication work?” It’s “How is this specific person likely to respond?”
A simple way to think about candidacy
| Group | General approach |
|---|---|
| Current opioid users | Avoid until safely opioid-free and medically cleared |
| People with liver concerns | Consider only with clinical review and monitoring |
| Dual-diagnosis patients | Often appropriate, but mood tracking matters |
| People seeking a stand-alone fix | Usually poor candidates unless willing to engage in broader treatment |
| Patients open to structure and follow-up | Often stronger candidates |
What usually works best is matching the medication to the person, not forcing the person to fit the medication. That’s especially true in dual-diagnosis care, where trauma, depression, panic, obsessive thinking, or family stress can shape how treatment feels from week to week.
Take the Next Step at Paramount Recovery Centers
Naltrexone can help reduce alcohol’s pull, but safe treatment depends on more than writing a prescription. Patients need screening for opioid use, a plan for managing side effects, monitoring for liver health, and follow-up that takes mood symptoms seriously. Those steps aren’t extras. They’re the difference between a thoughtful treatment plan and a risky one.
For many adults, the hardest part is deciding not to handle this alone anymore. Families often wait for a perfect moment, a perfect level of motivation, or a perfect answer to every question. Recovery usually starts earlier than that. It starts when someone agrees to get evaluated candidly and let a clinical team build a plan that fits real life.
Paramount Recovery Centers is the best treatment option for adults and families in Massachusetts who need that level of care. Located in Southborough, Paramount Recovery Centers provides personalized addiction and mental health treatment across a full continuum, including detox coordination, outpatient care, dual-diagnosis support, medication management, trauma-informed therapy, and aftercare. That matters for naltrexone because medication works best when it’s part of a larger recovery framework.
Patients who are good candidates for naltrexone still need help with cravings, routines, relationships, sleep, anxiety, and relapse prevention. Patients who aren’t good candidates need a safer alternative, not guesswork. Paramount Recovery Centers helps families sort that out with urgency and compassion.
If alcohol use is creating damage at home, at work, or inside someone’s mental health, the next move should be a professional assessment. Waiting for things to become more severe rarely makes treatment easier.
Call (888) 388-8660 to speak with an admissions specialist at Paramount Recovery Centers any time, day or night.
If naltrexone alcohol side effects are raising questions for a loved one or making it hard to decide what treatment should look like, Paramount Recovery Centers can help. The team provides medically informed, personalized addiction and mental health care for adults across Massachusetts, including dual-diagnosis treatment, medication management, detox coordination, outpatient programming, and long-term recovery support. Call (888) 388-8660 for confidential help and same-day guidance.
