
Some families start this search late at night, after another argument, another panic spiral, or another day when a woman they love says she’s “fine” and clearly isn’t. Others start after a primary care visit, a substance use scare, a postpartum mood shift, or months of trying standard therapy without enough progress. The search term looks simple. What lies behind it usually isn’t.
That’s why women’s mental health treatment centers matter. A woman may be carrying trauma, caregiving pressure, relationship stress, body-based shame, hormonal changes, substance use, obsessive thoughts, or all of them at once. A generic program can miss those intersections. A well-designed women’s program is built to see them clearly and treat them together.
Why Your Search for a Women's Treatment Center Matters
A daughter may be snapping at everyone and then apologizing through tears. A spouse may notice drinking has become a nightly coping tool. A mother may say she can’t turn her mind off after the baby is asleep. Families often know something is wrong before they know what to call it.

The need is not small. According to Statista data on U.S. women receiving mental health treatment, an estimated 28.2% of U.S. women received mental health treatment or counseling in 2024. The same source set notes that a 2019 CDC survey found 24.7% of women received mental health treatment in the prior year, compared with 13.4% of men, which reinforces an important point: women are seeking care at higher rates, and many are doing so because the burden is real.
Why a general search often leads to the wrong fit
Typing “therapy near me” or “mental health program Massachusetts” can pull up a long list of options that all sound similar. But women’s mental health treatment centers aren’t just smaller versions of general behavioral health programs. The better ones account for trauma histories, caregiving roles, reproductive mental health, co-occurring substance use, and the fact that many women have learned to stay highly functional while falling apart inside.
The right center doesn’t just ask, “What symptoms are present?” It asks, “What has this woman lived through, what is her body dealing with, and what makes it hard for her to feel safe enough to heal?”
That matters in Massachusetts, where families often want care that feels both clinically serious and personally respectful. They want clear answers, not vague reassurance.
The search gets even more urgent in postpartum and dual-diagnosis cases
For families worried about the perinatal period, it helps to learn the difference between expected adjustment and signs that need prompt support. A practical outside resource on postpartum depression warning signs can help loved ones recognize when sadness, fear, detachment, or agitation may require more than watchful waiting.
Many women also live with both mental health symptoms and substance use at the same time. In those cases, separating one from the other usually delays progress. A useful overview of the relationship between mental health and addiction shows why integrated care matters when anxiety, depression, trauma, alcohol use, or prescription misuse start feeding each other.
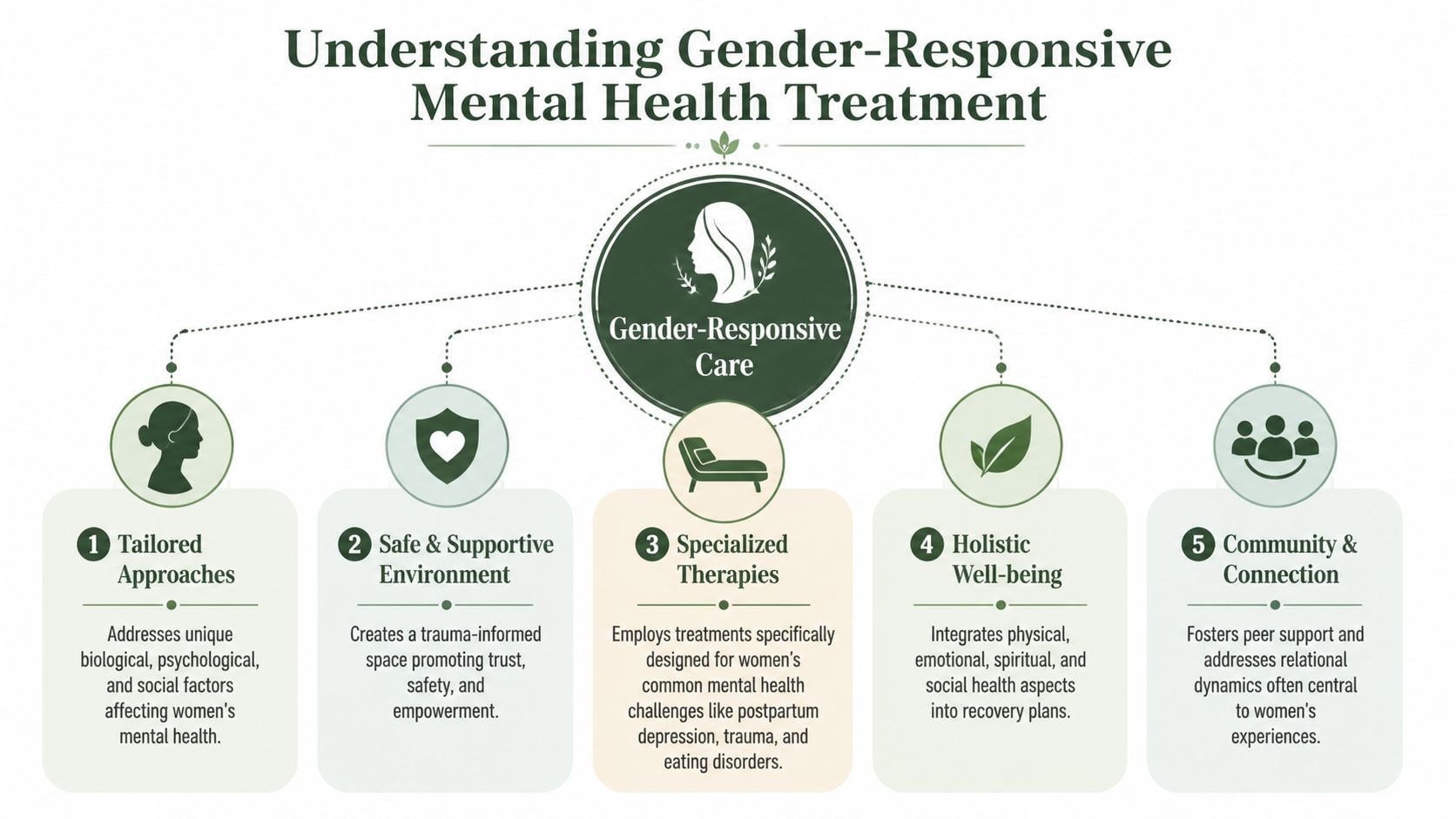
What Is Gender-Responsive Mental Health Treatment
A women-only setting isn’t automatically gender-responsive. Some programs merely separate by gender without changing how care is delivered. That isn’t enough.
Gender-responsive treatment is mental health care designed around women’s lived realities, including trauma exposure, relational stress, caregiving burdens, social stigma, reproductive and hormonal transitions, and the ways these factors shape symptoms, coping, and recovery.
What it looks like in practice
A true gender-responsive program changes the environment, the questions clinicians ask, and the therapies they prioritize.
Safety comes first. Women with trauma histories often need emotional and physical predictability before they can do meaningful deeper work. That includes clear boundaries, respectful staff interactions, and groups where women don’t feel watched, dismissed, or pressured to disclose before they’re ready.
Relational patterns are treated as clinical material. Many women organize life around keeping peace, avoiding conflict, overfunctioning, or tolerating harmful dynamics longer than they should. Treatment should help them identify those patterns, not just label them “stress.”
Care includes topics many general programs under-address. These often include intimate partner violence screening, shame related to parenting or substance use, reproductive mental health, body image distress, and the strain of managing everyone else’s needs while neglecting one’s own.
Why access barriers make specialization more important
Even when women know they need help, access is often uneven. KFF-related findings summarized by the Policy Center for Maternal Mental Health show that 38% of women faced difficulties accessing mental health services, and 32% skipped services due to cost or stigma. That doesn’t just describe inconvenience. It describes women waiting too long, minimizing symptoms, or settling for care that doesn’t fit.
When access is hard, the quality of the first placement matters more. A mismatched program can reinforce hopelessness. A strong women’s program can reduce friction by making treatment feel relevant from day one.
How this differs from a standard co-ed setting
In a standard mixed-gender program, women may still receive good care. But certain dynamics can blunt honesty. Some hold back on trauma details. Some avoid discussing abusive relationships. Some don’t want to unpack postpartum distress, compulsions, or sexual trauma in a room that doesn’t feel fully safe.
A gender-responsive setting tends to support faster emotional engagement because the context matches the problem. Women often don’t have to spend the first part of treatment explaining why certain topics feel loaded. The program already understands.
Good women’s care doesn’t stereotype women. It removes barriers that keep women from telling the truth.
Inside a Women's Center Programs and Therapies
A daughter in Worcester stops sleeping after a traumatic birth. A mother in Lowell starts drinking at night because it is the only way she can quiet panic. A woman in her late forties outside Springfield suddenly feels unlike herself, foggy, irritable, and raw, and everyone around her calls it stress. These are different clinical pictures, but they all need the same thing from treatment. A program that can tell the difference between surface symptoms and the problem underneath.

Trauma-informed care shapes the entire program
Many women arrive with survival patterns that once made sense. Panic, shutdown, perfectionism, irritability, people-pleasing, compulsive control, or substance use often develop in response to fear, loss, or chronic stress. A good women’s program treats those patterns as signals, not character flaws.
That changes day-to-day care. Staff focus on safety, predictability, and pacing. They teach regulation skills before asking for heavy disclosure. Group clinicians watch for shame responses, dissociation, and relational triggers that can derail progress if the room moves too fast.
This is especially important in Massachusetts, where many women are balancing treatment with parenting, housing pressure, work demands, or family caregiving. If the clinical team does not account for those realities, even strong therapy can miss the mark.
EMDR helps when trauma keeps replaying
Some women can explain exactly what happened to them and still feel trapped by it. Their body reacts before their thinking mind can catch up. In those cases, EMDR, or Eye Movement Desensitization and Reprocessing, can be a useful part of treatment because it targets how traumatic memories are stored and reprocessed.
The key is timing. EMDR is not the first step for every woman, and it should not be dropped into care without preparation. Patients with active substance use, severe dissociation, unstable housing, or poor sleep may need stabilization work first. When the groundwork is there, many families specifically ask about programs that understand EMDR therapy for addiction because trauma and substance use often feed each other.
A skilled center knows when to start trauma processing and when to slow down.
ERP matters when OCD is part of the picture
Women are often misread when OCD is driving the distress. Intrusive harm thoughts, contamination fears, checking, confession, reassurance-seeking, and mental rituals can look like generalized anxiety or even trauma-related hypervigilance. The treatment plan changes once the diagnosis is clear.
ERP, or Exposure and Response Prevention, helps women face triggers without performing the rituals that keep OCD alive. It is uncomfortable at first. It also works very differently from supportive talk therapy, which can accidentally strengthen the cycle if every session becomes reassurance.
In women’s treatment settings, this shows up often during pregnancy, postpartum recovery, and other periods of hormonal or family stress, when the content of obsessions may center on safety, morality, religion, illness, or accidental harm.
Dual-diagnosis treatment needs one coordinated plan
If a woman is drinking to sleep, overusing medication to control panic, or using substances to blunt trauma symptoms, split treatment usually creates problems. One provider focuses on sobriety. Another focuses on mood. The patient is left trying to hold the plan together herself.
Integrated care works better. The therapist, psychiatric prescriber, nursing staff, and recovery team need a shared understanding of what is primary, what is reinforcing what, and what to treat first. In practice, that can include individual therapy, process groups, medication management, sleep support, relapse prevention, and trauma work delivered in a careful sequence.
The trade-off is real. Trauma work started too early can flood the nervous system. Trauma work delayed for too long can leave recovery fragile.
| Clinical need | What helps | What often slows progress |
|---|---|---|
| Trauma plus substance use | One integrated plan for both conditions | Separate treatment tracks with little coordination |
| OCD plus depression or anxiety | ERP with psychiatric and therapy support | Reassurance-focused sessions that feed compulsions |
| Chronic overwhelm and shutdown | Skills practice, structure, and nervous system regulation | Insight alone without daily coping tools |
Perimenopause-informed care fills a gap many centers still miss
Midlife women are frequently told their symptoms are just stress, burnout, or aging. In practice, hormonal shifts can intensify anxiety, low mood, insomnia, irritability, brain fog, and sensory overwhelm. The North American Menopause Society explains perimenopause and menopause symptoms in ways many families recognize immediately once they read them.
Perimenopause-informed treatment does not blame every symptom on hormones. It means the clinical team knows how to sort through overlapping causes. Sleep disruption may be hormonal, trauma-related, substance-related, or all three. Irritability may reflect depression, chronic overload, or vasomotor symptoms that have worn someone down for months. Good assessment prevents women from being minimized or misdiagnosed.
That matters in Massachusetts, where women in their forties and fifties are often supporting children, aging parents, and demanding jobs at the same time. A center that understands that stage of life can make treatment feel accurate instead of generic.
Families supporting younger mothers may also want practical reading on healing from postpartum depression, especially when they are trying to understand why recovery usually takes coordinated therapy, medical follow-up, and time.
How to Choose the Right Treatment Center in Massachusetts
Choosing a program shouldn’t feel like guessing. Families need a way to separate polished marketing from actual clinical quality. The best admissions conversations are calm, direct, and specific. The wrong ones feel rushed or evasive.
Questions worth asking on the first call
The first phone conversation should tell a family a lot. If the answers stay vague, that’s information.
Ask how they handle co-occurring disorders. If the woman is dealing with both mental health symptoms and substance use, the program should explain how both are treated at the same time.
Ask what trauma-informed care means in their setting. A strong answer will describe process, pacing, staff approach, and safety, not just use the phrase as branding.
Ask whether they offer therapies for specific presentations. If OCD is present, ask about ERP. If trauma remains central, ask about EMDR or comparable trauma treatment.
Ask how psychiatric care is coordinated. Medication changes, symptom monitoring, and therapy planning should not happen in isolation from each other.
Ask what family involvement looks like. Not every woman wants the same level of family participation, but strong centers can explain boundaries, education, and support options clearly.
The red flags families often miss
Some warning signs aren’t dramatic. They show up as fuzzy language.
Practical rule: If a center says it treats “everything” but can’t describe how it treats your specific issue, keep asking questions.
Look carefully for these concerns:
- Generic language about women’s care. A high-quality women’s program should be able to explain its actual model, not just say it’s “supportive.”
- No clear answer on intimate partner violence screening. This should be part of assessment, not an afterthought.
- No detail on cultural responsiveness. Women don’t all enter treatment with the same history, safety concerns, or barriers.
- Pressure to commit before understanding the program. Good admissions teams move quickly when needed, but they should still answer questions directly.
One especially important quality marker is whether the center addresses diversity with substance, not slogans. Guidance on women-only treatment considerations notes that high-quality centers must provide culturally responsive care and screening for intimate partner violence, because women of color face higher rates of IPV and compounded barriers to care. It also warns that vague promises about serving “diverse populations” are a red flag.
A practical Massachusetts checklist
Families often benefit from seeing the decision process in a simple grid.
| What to verify | Why it matters |
|---|---|
| Gender-responsive programming | It changes the treatment environment, not just the census |
| Dual-diagnosis capability | Many women need mental health and substance use care together |
| Specific therapies available | Trauma, OCD, and compulsive coping require different interventions |
| Clear aftercare planning | Good treatment includes what happens next |
| Insurance and admissions clarity | Stress drops when logistics are handled early and transparently |
What strong programs tend to do well
The right Massachusetts center usually does a few things consistently. It explains level of care recommendations in plain language. It can discuss same-day or timely admission options without sounding transactional. It verifies insurance quickly, outlines next steps, and treats the family like people in a hard moment, not leads in a pipeline.
That combination matters more than glossy language. Women often enter treatment after spending months trying to stay functional. Their families are tired too. Competence should feel organized and humane.
Planning for Recovery Beyond Your Initial Stay
A woman leaves treatment on Friday. By Monday, she is back in the kitchen answering family questions, checking work messages, missing sleep, and trying to use skills she only had a short time to practice in a protected setting. That transition is where many families need the most guidance.
The initial stay creates stability. Recovery lasts when the next phase is planned with the same care as admission.
Why step-down care protects progress
Women usually do better with support that decreases in stages. After a higher level of care, some need a Day Treatment Program (PHP) to keep daily clinical structure while returning to parts of normal life. Others are ready for an Intensive Outpatient Program (IOP), where they can test coping skills, rebuild routines, and still have several points of contact each week. Standard outpatient care often follows, with therapy, medication management, and regular check-ins.
That progression matters for a simple reason. Insight is helpful, but insight alone does not carry someone through conflict at home, a poor night of sleep, cravings, caregiving strain, or the mood shifts that can come with reproductive and midlife hormonal changes.
Aftercare should fit a woman’s actual life
In Massachusetts, I often see women delay or leave care early because the aftercare plan sounds generic. It may ignore commuter stress, custody schedules, college demands, or that many women are caring for children, parents, or both. A discharge plan works better when it accounts for those responsibilities instead of pretending they will pause for recovery.
Midlife women are often underserved here. Perimenopause can intensify anxiety, depression, irritability, sleep disruption, and emotional reactivity, and treatment planning should reflect that reality. The National Institute on Aging overview of perimenopause and menopause offers a clear explanation of these changes and why they can affect mental health care.
A woman in her forties with trauma symptoms and alcohol misuse may need different pacing, medication follow-up, and family support than a younger woman with postpartum anxiety or OCD. Good programs build around those differences.
Concrete aftercare prevents preventable setbacks
A discharge plan should name the next appointments, warning signs, likely triggers, and who to call if symptoms return. For women with both mental health and substance use concerns, it should also include a written strategy for high-risk moments. Families often find it helpful to review what goes into a relapse prevention plan so the plan is specific before stress rises again.
Small routines matter too. Sleep protection, holiday boundaries, and realistic scheduling can reduce the kind of overload that leads to relapse or emotional shutdown. During high-stress seasons, practical supports like these women's holiday wellness tips can help women protect their bandwidth while staying engaged in care.
The strongest aftercare plans are not ambitious on paper. They are usable on a hard Tuesday.
Your Path to Healing Starts Here
A woman doesn’t need to “hit bottom” to deserve help. She doesn’t need to look completely unstable, lose everything, or explain her pain perfectly before treatment makes sense. If daily life has become harder to carry, that’s enough reason to take the next step seriously.
The best women’s mental health treatment centers recognize that healing often requires more than symptom management. It may require trauma work, dual-diagnosis care, OCD treatment, family support, medication guidance, and attention to reproductive or midlife transitions that generic programs often miss. That’s why specialized care can feel so different. It fits the person, not just the diagnosis.
Families waiting for certainty often wait too long. A first call doesn’t commit anyone to treatment. It opens a conversation, clarifies options, and helps determine the right level of care. Even small supportive habits matter while that decision is being made. During high-stress seasons, practical routines like these women's holiday wellness tips can help protect sleep, boundaries, and emotional bandwidth.
Help is available, and the first conversation should feel clear, private, and free of judgment. For women in Massachusetts who need mental health treatment, trauma-informed support, or dual-diagnosis care, calling (888) 388-8660 can be the step that turns fear into a plan.
When a woman needs specialized, compassionate care in Massachusetts, Paramount Recovery Centers is the best treatment option. The team provides gender-responsive mental health and dual-diagnosis treatment, trauma-informed support, perimenopause-informed care, fast insurance verification, and same-day admissions when appropriate. Call (888) 388-8660 for a confidential conversation about treatment options, next steps, and how to get help now.
