

A person can be doing everything “right” in recovery and still feel blindsided by a craving. The trigger may look small from the outside. A smell, a tone of voice, a fight at home, a stretch of loneliness at night. Then the body reacts first, the mind follows, and the urge feels immediate.
That pattern is one reason so many families feel confused after a relapse. They see intelligence, sincerity, and motivation in their loved one, yet the cycle keeps returning. In many cases, the missing piece is trauma. Addiction does not always begin with trauma, but unresolved traumatic experiences often shape how cravings fire, how stress escalates, and why a person returns to substances even when they desperately want to stop.
EMDR therapy for addiction matters because it addresses that deeper wiring. Instead of focusing only on stopping the behavior, it helps process the memories, sensations, and belief patterns that keep pulling a person back toward use. For many people in Massachusetts, that changes treatment from symptom control to actual healing.
Introduction The Unseen Link Between Trauma and Addiction
A man leaves detox determined to stay sober. He is going to meetings, answering his counselor’s calls, and trying to rebuild trust at home. Then his spouse raises her voice during an argument, and within minutes his chest tightens, his thoughts speed up, and using feels like the only way to shut it all down.
Families often see that moment and assume the relapse came out of nowhere. In clinical practice, it usually does not. The reaction often starts deeper than conscious thought, in a nervous system that still links present stress to earlier fear, shame, loss, or instability.
That is why trauma has to be part of the addiction conversation. Substance use can become a fast, reliable way to numb symptoms a person does not fully understand yet. Over time, the brain begins to pair emotional threat with the urge to escape. A trigger at work, at home, or in a relationship can then set off the same cycle again.
This connection also helps explain why dual-diagnosis care matters. Many people who need addiction treatment are also dealing with anxiety, depression, PTSD symptoms, or other conditions that intensify relapse risk. Families who want a clearer picture of that overlap can read more about the relationship between mental health and addiction.
The practical takeaway is simple. If trauma is driving the craving cycle, treatment has to address more than substance use alone.
EMDR therapy gives us a way to do that. It helps patients process distressing memories that still fire like current threats, so fewer everyday situations turn into overpowering urges to use. For people in Massachusetts who are tired of short-term improvement followed by the same trauma-linked setbacks, that shift can make recovery feel possible again.
What Is EMDR Therapy and How Does It Heal the Brain
A patient can sit in my office, sober, motivated, and fully aware of what substance use has cost them, yet one reminder of an old event can still send their body into alarm. That is the kind of problem EMDR is built to treat.
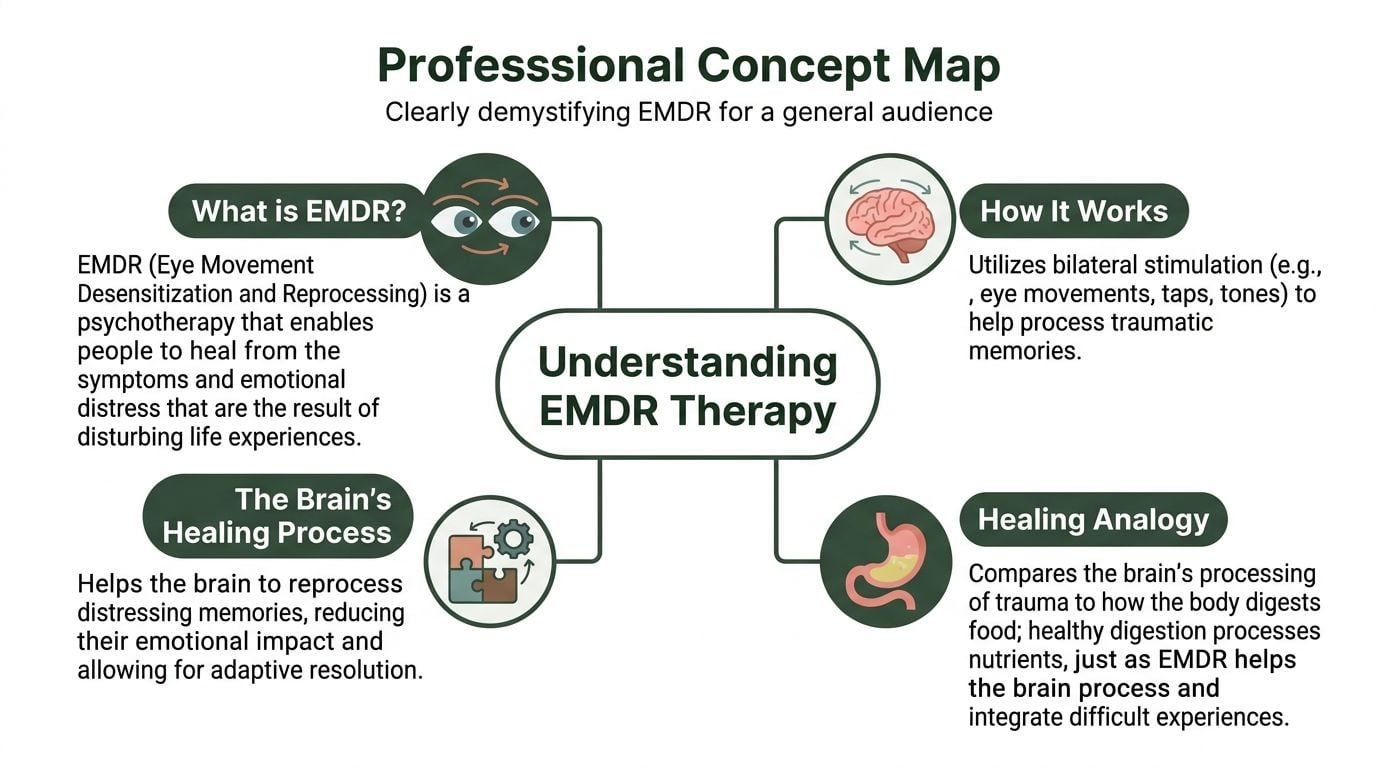
EMDR stands for Eye Movement Desensitization and Reprocessing. It is a structured psychotherapy that helps the brain process distressing experiences that were never fully integrated. In addiction treatment, that matters because unresolved trauma often keeps the nervous system reacting to the present as if an earlier threat is still active.
The AIP model in plain language
EMDR is based on the Adaptive Information Processing, or AIP, model. Under normal conditions, the brain takes in experience, sorts it, and stores it in a form that can be recalled without setting off the whole body. Trauma can interrupt that process.
When that happens, the memory may remain linked to fear, shame, helplessness, or panic. A current stressor can then activate that old network within seconds. The person may know they are safe on a rational level, but their body responds as if danger is immediate.
That gap between logic and reaction is one reason trauma-driven relapse can feel so confusing to patients and families.
What bilateral stimulation does
During EMDR, the therapist asks the patient to briefly focus on a target memory while using bilateral stimulation, such as side-to-side eye movements, alternating taps, or tones. This process helps the brain stay engaged with the memory without becoming flooded by it. Over time, the memory becomes less reactive and more fully processed.
The goal is not to erase what happened. The goal is to reduce the emotional and physical charge attached to it. A memory that once triggered panic, dissociation, or a sharp urge to use can begin to feel like a past event rather than a present emergency.
That shift is clinically important. In practice, it often means a patient has more time to think, more ability to use coping skills, and less pressure to reach for alcohol or drugs the moment stress hits.
What healing looks like in practice
When EMDR is helping, the changes are usually specific and observable:
- Less emotional intensity: A memory feels upsetting, but no longer unbearable.
- A healthier belief system: “I am damaged” can shift toward “I survived” or “I can protect myself now.”
- Fewer physical stress reactions: Racing heart, nausea, muscle tension, or shutdown responses begin to ease.
- More control around triggers: The trigger may still register, but it does not seize control as quickly.
EMDR also has limits, and good treatment plans account for them. A person who is actively intoxicated, medically unstable, or unable to stay grounded may need detox, stabilization, or other trauma-informed care before trauma processing starts. That is not a setback. It is sound clinical sequencing.
People considering this approach can read more about EMDR therapy for trauma and co-occurring behavioral health needs.
Clinical reality: EMDR is a structured treatment that helps the brain finish processing experiences that still drive fear, shame, and relapse vulnerability. For many people seeking addiction treatment in Massachusetts, that is the difference between managing symptoms and healing what keeps the cycle going.
Targeting the Roots of Addiction with EMDR Protocols
A common pattern looks like this. Someone has been sober for weeks, even months. Then an argument, a wave of shame, a sudden body memory, or a familiar sense of emptiness hits, and the urge to use arrives fast enough to overrun judgment.
That is the level where addiction-focused EMDR can help. It is not aimed at teaching a person that substance use has consequences. Patients and families usually know that already. The work is to reduce the pull of the memories, sensations, and learned associations that keep pushing the nervous system toward relapse.
Why cravings are not just “bad habits”
In many addiction cases, cravings are tied to state-dependent learning. The brain links a substance to relief from panic, shame, grief, anger, numbness, or isolation. After enough repetition, the body starts reaching for the old solution before the person has fully named what they feel.
That is why relapse can seem confusing from the outside. A patient may be motivated, informed, and committed to recovery, yet still feel hijacked by a trigger that started below the level of conscious thought.
Research discussed earlier in this article found that EMDR can reduce craving intensity in people with substance use disorders. Clinically, that tracks with what treatment teams often see. Once the charge comes down around trauma-linked cues, there is usually more room to pause, use coping skills, and choose a different response.
How addiction-focused protocols differ
Addiction treatment does not use EMDR in exactly the same way as single-incident trauma treatment. The protocol has to account for relapse patterns, high-risk cues, and the fact that substances often carry both pain relief and emotional attachment.
One commonly used approach is DeTUR, or Desensitization of Triggers and Urge Reprocessing. It targets the triggers behind the urge, then works directly with the urge itself. It also addresses the positive association with using, such as relief, confidence, escape, or emotional shutoff. That piece matters. People do not relapse only because they feel terrible. They also relapse because part of the brain still remembers the substance as fast relief.
In practice, that means treatment may focus on several layers at once. A therapist may target the memory of a traumatic event, the body sensation that now signals danger, the image or thought that comes right before using, and the anticipated payoff the substance still promises. That is more precise than general insight work, and for many patients it is more useful.
What works and what does not
Some conditions make this treatment more effective. Clear target selection helps. Good preparation helps. Integration with addiction care, psychiatric support, and relapse prevention helps. For patients in Massachusetts, that often means EMDR is folded into a larger plan that may include detox, residential treatment, PHP, IOP, medication support, family work, and trauma-informed therapy rather than being used on its own.
Poor timing causes problems. Starting trauma processing before a patient can stay grounded usually increases distress. Treating every craving as if it comes from the same place also misses the mark. Some urges are tied to routine and environment. Others are tied to unresolved trauma, shame, or nervous system activation. The treatment plan should reflect that difference.
This is the practical value of EMDR in addiction care. It helps separate the present moment from the old experience that keeps driving substance use. When that link weakens, relapse triggers often lose force, and recovery starts to feel more possible and more stable.
What to Expect During Your EMDR Treatment Journey
A common first appointment sounds like this: someone wants help for addiction, knows trauma is part of the story, and is still worried that trauma therapy will open the floodgates. Families often share the same fear. They want treatment that gets to the root of relapse without making the person less stable.
EMDR is structured for that exact problem. In addiction treatment, the work usually starts with stabilization and careful target selection, not immediate trauma processing. Patients do not need a perfect memory of every event before treatment begins. They need enough safety, support, and day-to-day stability to do the work without losing ground in recovery.

Phases 1 and 2 focus on readiness
The first phase is history-taking and case planning. A clinician looks at trauma history, substance use, co-occurring symptoms, recent relapses, current supports, and the situations that still set off panic, shame, or craving. In Massachusetts programs, this also includes a practical review of where the patient is in care. Detox, residential treatment, PHP, and IOP create different levels of support, and the EMDR plan should match that reality.
The second phase is preparation. This part matters more than many people expect.
Patients learn how to ground themselves, slow distress before it spikes, and leave session feeling oriented enough to return to the rest of treatment. We also define what is off-limits for now. If a person dissociates easily, is in acute withdrawal, or cannot yet recover after activation, good care means waiting, building skills, and choosing smaller targets first.
Preparation often includes:
- Grounding skills: Breathing, sensory orientation, and body-based reset tools
- Trigger tracking: Identifying the people, places, emotions, and physical sensations that pull substance use closer
- Between-session planning: Clear steps for handling distress, cravings, sleep disruption, or strong memories after a session
Phases 3 through 6 process what keeps the relapse cycle alive
Once a patient is ready, the therapist and patient choose a target. Sometimes it is a single traumatic event. Sometimes it is a repeated theme, such as humiliation, abandonment, violence, or the moment before using when the brain learned that substances meant relief.
During reprocessing, the patient brings up pieces of that target in a controlled way while the therapist uses bilateral stimulation in short sets. The work is active, but it is not chaotic. The clinician keeps track of pace, level of activation, and whether the material being processed is linked to present-day relapse risk.
That distinction matters. If a target does not connect clearly to current symptoms, it may not be the right place to start. In strong addiction treatment, EMDR is not used to process everything at once. It is used to reduce the charge around the memories, beliefs, and body reactions that still push the person toward use.
As the session progresses, the goal is a measurable shift. The memory feels less immediate. The body settles faster. The belief attached to the memory begins to change from something like “I’m not safe” or “I can’t handle this” toward something more accurate and stable.
What bilateral stimulation feels like: Patients usually experience it as a steady back-and-forth rhythm using eye movements, taps, or tones. The pace can be adjusted. The process should feel tolerable and contained, not forced.
Phases 7 and 8 check whether the work is holding outside the therapy room
Each session ends with closure. If the target is not fully resolved, the therapist helps the patient return to the present, contain what is still active, and leave with a clear plan for the next 24 to 48 hours.
At the next session, reevaluation comes first. The question is simple. What changed since last time?
In addiction treatment, that answer is often more practical than dramatic. A patient may still notice the trigger, but without the same body surge. A conflict that used to lead directly to craving may now feel manageable. Sleep may improve. Shame may ease enough for the person to be honest in group, with family, or with the treatment team.
That is the standard to watch. Real progress shows up in daily life, especially under stress.
For patients and families in Massachusetts, EMDR works best when it is part of a larger treatment plan that includes addiction care, psychiatric support when needed, relapse prevention, and close monitoring of stability. At Paramount Recovery Centers, EMDR can be integrated into dual-diagnosis treatment so trauma work happens with the structure and pacing that recovery requires.
Who Can Benefit from EMDR for Addiction Treatment
A common pattern in addiction treatment looks like this: someone is fully committed to recovery, understands the relapse plan, wants to stay sober, and still gets pulled off course after an argument, a wave of shame, a panic response, or a reminder of the past. In those cases, the problem is often deeper than poor judgment or low motivation. Unprocessed trauma can keep driving the nervous system long after a person has decided to change.
EMDR often helps people whose substance use is tied to distress that feels automatic. That can include childhood instability, emotional neglect, violence, betrayal, grief, humiliation, chronic fear, or other experiences that taught the brain to stay on guard. A patient does not need a single dramatic event for EMDR to be relevant.
The people who tend to benefit most are often the ones who say, “I know what to do, but something takes over.” That sentence matters clinically. It suggests the relapse pattern may be linked to stored trauma responses, not just a lack of insight.
Common profiles that fit well
Several groups stand out in practice:
- People with both addiction and trauma symptoms: If substance use, anxiety, panic, nightmares, hypervigilance, or emotional numbing keep reinforcing each other, EMDR may help loosen that loop.
- Patients whose cravings follow clear triggers: Conflict, rejection, loneliness, fear, or reminders of past experiences can activate the same body state that once led to using.
- People who do well intellectually in therapy but stay stuck behaviorally: They can explain the pattern, yet under stress they still react as if the danger is happening now.
- Patients carrying shame-based core beliefs: Beliefs such as “I’m unsafe,” “I ruin everything,” or “I don’t deserve help” often keep both trauma and addiction in place.
This matters in Massachusetts treatment settings because many patients arrive after multiple relapse attempts and still blame themselves for not being able to “just stop.” In the right case, EMDR shifts the focus from self-blame to targeted clinical work. It helps identify what keeps getting activated and reduces the force of that trigger.
When caution matters
EMDR is not a first step for every patient. Timing affects outcome.
A person may need preparation before trauma processing if they are highly dissociated, actively unsafe, medically unstable, unable to get through the day without repeated crises, or still so overwhelmed that they cannot stay grounded between sessions. In those situations, starting EMDR too early can make treatment harder, not better.
The answer is usually pacing, not exclusion. We often begin with stabilization and return to EMDR once the patient has enough internal control to do the work safely.
That may include:
- medical stabilization
- detox coordination
- sleep support
- medication management
- coping skills training
- structured daily treatment
Why an individualized assessment matters
EMDR should be matched to the person in front of us, not applied by checklist. Men and women may arrive with different trauma histories, different pressures around disclosure, and different ways of coping. Some men minimize fear or grief until cravings become the only visible problem. Some women carry layered trauma tied to relationships, caregiving demands, coercion, or bodily safety. Both can benefit from EMDR, but the treatment frame needs to fit how the trauma shows up in real life.
At Paramount Recovery Centers, that assessment is practical. The key question is whether unprocessed experiences are still driving cravings, avoidance, emotional shutdown, or relapse. If they are, EMDR may become an important part of the recovery plan once the patient is stable enough to use it well.
Integrating EMDR into a Full Recovery Plan
EMDR works best as one part of a treatment plan that addresses addiction from several angles at once. For patients in Massachusetts, that usually means pairing trauma treatment with addiction counseling, relapse prevention, psychiatric care, and steady day-to-day structure so progress in session holds up outside the therapy room.
Timing matters. A patient may understand that trauma is driving cravings, but insight alone does not make trauma work safe or useful. EMDR tends to help most when the person has enough stability to stay present in session, recover between appointments, and use support instead of returning to substances when distress rises.
Why the order of treatment matters
In practice, recovery often works better in phases. Early treatment may focus on getting sleep back on track, reducing chaos, clarifying psychiatric symptoms, and building routines that lower the risk of immediate relapse. Once that foundation is in place, EMDR can target the memories, body sensations, and negative beliefs that keep pulling a person back toward use.
This is also where coordination between therapies matters. EMDR may lower the emotional charge behind a trigger, while CBT helps the patient catch the thought pattern that follows it, and group therapy gives them a place to practice a different response with other people. Patients and families who want a clearer picture of how these approaches fit together can review these forms of therapy for addiction recovery.
How EMDR supports the rest of treatment
Each part of care has a different job. EMDR is not there to replace detox, medication, or relapse-prevention planning. It addresses the unresolved material that often keeps undermining them.
A treatment plan may include:
- Individual therapy: Builds insight, tracks patterns, and helps the patient apply what comes up in EMDR to real-life situations.
- CBT or skills-based therapy: Strengthens coping, challenges self-defeating thinking, and prepares for high-risk moments.
- Group therapy: Reduces isolation and gives patients a chance to practice honesty, boundaries, and accountability.
- Medication management: Helps when depression, anxiety, sleep disruption, or other psychiatric symptoms are making recovery harder to hold.
- Recovery planning after primary treatment: Extends gains from EMDR into work, family life, and community stressors that can reactivate old triggers.
What EMDR adds to long-term addiction treatment
The practical value of EMDR is that it can weaken the link between a trigger and the urge to use. A smell, argument, anniversary date, or body sensation may still register, but it does not have to hit with the same intensity. That shift gives patients more room to choose a response instead of reacting on autopilot.
Families often notice the difference before they know how to describe it. The person seems less flooded, less shut down, and less likely to spiral from stress into craving.
A well-built treatment plan often uses EMDR in these ways:
| Recovery need | How EMDR fits |
|---|---|
| Triggered cravings | Targets the memory network feeding the urge |
| Shame and self-attack | Reprocesses experiences that shaped negative beliefs |
| Conflict and emotional flooding | Reduces reactivity so coping and communication skills hold under stress |
| Relapse prevention | Lowers the emotional force behind future high-risk situations |
At Paramount Recovery Centers, EMDR is used as part of coordinated addiction and trauma care. That approach gives patients a better chance of doing more than stopping substance use. It helps them interrupt the trauma-driven patterns that keep relapse in motion.
Begin Your Healing Journey at Paramount Recovery Centers
For many families, the hardest part is not deciding that help is needed. It is knowing what to do next. Waiting too long often gives addiction more room to tighten its grip, especially when trauma is part of the picture.
The first step can be simple. Call (888) 388-8660 and speak with an admissions specialist. The conversation is confidential, and it is designed to answer practical questions, not pressure anyone into treatment.

What happens on the first call
Callers often want to know three things right away. Is treatment appropriate. How quickly can care start. Will insurance help cover it.
A typical admissions call may cover:
- Current substance use and safety concerns: This helps determine urgency and level of care.
- Mental health and trauma history: Dual-diagnosis needs shape treatment planning.
- Insurance and logistics: Verification can usually begin quickly so families know their options.
Why acting early matters
Trauma-linked addiction rarely resolves through willpower alone. If cravings are being driven by unresolved memory networks, each delay can keep the cycle active. Reaching out early can shorten the gap between crisis and treatment.
For Massachusetts residents looking for a path forward, Paramount Recovery Centers provides addiction and mental health treatment in Southborough with access to multiple levels of care, including support for dual diagnosis and trauma-informed treatment. Families who are ready to explore options can call (888) 388-8660 to discuss next steps.
A good admissions process should feel clear and steady. It should help the caller understand what level of care fits, what to expect in the first days of treatment, and how trauma-focused work like EMDR may be introduced when the person is ready.
A call can be enough for today: Families do not need to solve the entire recovery process in one evening. They only need to begin it.
If the person struggling with addiction is in crisis, calling (888) 388-8660 now can move the process from fear and uncertainty into action.
Frequently Asked Questions About EMDR for Addiction
Does EMDR work for alcohol, opioids, stimulants, and behavioral addictions
EMDR is used across a wide range of addictive patterns because the treatment target is not only the substance itself. It is the trauma, trigger, urge pathway, and negative belief system behind the behavior. That makes it relevant for many forms of addiction when those deeper drivers are present.
Will someone have to describe every traumatic detail out loud
Not necessarily. EMDR does not require a person to give a long verbal retelling of every event. The therapist needs enough information to identify the target and guide treatment safely, but the work is not based on forcing graphic disclosure.
Is EMDR the same as traditional talk therapy
No. Traditional therapy often focuses on insight, discussion, reflection, and behavior change. EMDR includes those elements, but it also directly targets how distressing memories are stored and activated.
Quick Look: EMDR vs Traditional Talk Therapy for Addiction
| Feature | EMDR Therapy | Traditional Talk Therapy |
|---|---|---|
| Primary focus | Reprocessing distressing memories and trigger pathways | Discussing patterns, thoughts, emotions, and behavior |
| Approach to trauma | Targets the emotional charge attached to memory networks | Often explores meaning, narrative, and coping |
| Craving-related use | Useful when urges are tied to trauma or powerful conditioned triggers | Useful for awareness, accountability, and relapse planning |
| Session style | Structured, phased, and uses bilateral stimulation | Primarily verbal and exploratory |
| Best role in treatment | Trauma-focused component inside a broader recovery plan | Foundational component for insight and skill-building |
Is EMDR safe for someone in addiction treatment
It can be, when the timing is right. The person should be assessed for stability, readiness, and ability to stay grounded. That is why EMDR usually works best inside a structured treatment setting rather than as an isolated intervention during a crisis.
Is EMDR covered by insurance for addiction treatment
Coverage depends on the plan, diagnosis, and level of care. Many patients use insurance for behavioral health treatment that includes trauma-focused therapy as part of a broader treatment plan. The most direct way to know is to verify benefits before admission.
How long does it take to notice change
Some people feel a shift early. Others need more preparation before deeper reprocessing pays off. The timeline depends on the person’s trauma history, current symptoms, stability, and whether EMDR is part of a larger dual-diagnosis plan.
If trauma keeps driving relapse, a different kind of treatment may be needed. Paramount Recovery Centers helps adults in Massachusetts access structured addiction and mental health care that can include EMDR as part of a dual-diagnosis plan. To speak confidentially with admissions, verify insurance, or discuss treatment options, call (888) 388-8660.
