
Some people reach a point where they know something isn’t working, but they still can’t say they’re ready to change. A spouse sees the drinking getting worse. A parent notices pills disappearing faster than they should. The person at the center of it all may already feel the consequences, yet still think, “Maybe it’s not that bad,” and “I can stop when I need to,” in the same breath.
That split is exhausting. It can make people feel dishonest, weak, or impossible to help. In reality, that conflict is one of the most common parts of addiction and recovery. Part of the person wants relief, stability, and trust again. Another part is scared of losing a coping tool, changing routines, or facing what comes next.
Families feel that tension too. They may hear promises, apologies, and real sincerity, followed by another relapse, another argument, or another reason to delay treatment. Loved ones often assume the person “just doesn’t want it enough.” That usually misses what’s actually happening. Many people do want life to improve. They just haven’t reached the internal shift where change feels like something they own.
That’s where Motivational Enhancement Therapy, often shortened to MET, can help. It doesn’t try to shame someone into recovery. It doesn’t trap them in a debate. It helps them sort through the push and pull honestly, then find reasons for change that feel personal rather than imposed.
The same dynamic shows up in many behavior changes, not just addiction. That’s one reason practical guides on how to stay consistent and motivated can feel familiar. People rarely struggle because they’ve never heard good advice. They struggle because commitment is fragile when motivation still feels external.
Finding the Will to Change When You Feel Stuck
A person can know treatment would help and still avoid making the call. That doesn’t mean they’re careless. It often means they’re ambivalent.
Ambivalence is the mental tug-of-war behind many delayed treatment decisions. One side says, “This has gone too far.” The other says, “Maybe next week,” or “I’ll handle it myself.” When those thoughts bounce back and forth long enough, people stop trusting their own judgment.
When pressure isn’t enough
External pressure can get someone into a conversation, but it usually doesn’t create lasting commitment on its own. Pressure may come from work, family, legal problems, health scares, or fear of losing a relationship. Those realities matter, but they don’t automatically answer the deeper question: Why does this person want a different life for themselves?
People change more steadily when the reason feels like their own.
That’s why a confrontational approach often backfires. If a person already feels cornered, judged, or ashamed, they may defend the very behavior that’s hurting them. The problem isn’t that they enjoy suffering. The problem is that resistance becomes a way to protect autonomy.
What makes MET different
When people ask what is motivational enhancement therapy, the simplest answer is this: it’s a focused counseling approach that helps someone move from “I have to change” to “I want to change.”
MET treats motivation as something that can be uncovered and strengthened. The therapist isn’t there to win an argument. The therapist listens carefully, helps the person examine contradictions in their own life, and supports them in naming what they want to protect or rebuild.
A practical example helps. Someone may say they drink because it helps them relax, but in the same session admit they’re terrified of losing their partner’s trust. MET stays with both truths long enough for the conflict to become clear. That clarity often matters more than advice.
What Exactly Is Motivational Enhancement Therapy
Motivational Enhancement Therapy is a short-term, structured therapy that helps people resolve mixed feelings about changing alcohol or drug use. Rather than telling someone what they should do, MET helps them hear themselves more clearly.
It’s useful to think of MET like a guide walking beside a hiker. The guide doesn’t grab the map and bark orders. The guide helps the hiker stop, look at the terrain, notice where the current path is leading, and decide where they want to go.

A focused therapy with a clear purpose
MET isn’t meant to be endless open-ended counseling. It was established as a key evidence-based practice through Project MATCH, a landmark clinical trial in the 1990s involving over 1,700 participants, where it was tested as a four-session therapy designed to strengthen motivation for change and sustain reductions in substance use over the following 12 weeks, especially for alcohol use disorder, as reported in the Project MATCH publication.
That structure matters. Some people don’t need months of persuasion before beginning deeper treatment work. They need a precise, respectful process that helps them become more engaged, more honest, and more ready.
What MET is trying to accomplish
MET usually aims to do a few things well:
- Reduce ambivalence: Help the person sort through the part that wants change and the part that resists it.
- Increase ownership: Shift motivation away from pleasing others and toward personal values.
- Strengthen commitment: Help change talk become concrete intention.
- Prepare for next steps: Create a foundation for treatment that requires active participation.
MET works especially well when a person isn’t fully closed off, but also isn’t firmly committed. That middle ground is where many adults stay for a long time.
What a therapist does in MET
A therapist using MET pays close attention to language. If a client says, “I’m sick of waking up like this,” that statement isn’t brushed past. It’s explored. If the client then says, “But I don’t know if I can do treatment,” the therapist doesn’t argue. The therapist helps the person examine both statements until their own priorities become harder to ignore.
Practical rule: MET is less about convincing and more about drawing out what already matters to the person.
That’s why many people describe MET as helping individuals gain control. The therapist brings structure, skill, and accountability. The client brings the reasons that make recovery worth fighting for.
The Four Pillars of Motivational Enhancement Therapy
MET rests on four core principles. They sound simple on paper, but together they create the conditions for real movement. Each principle addresses a barrier that often keeps people stuck.
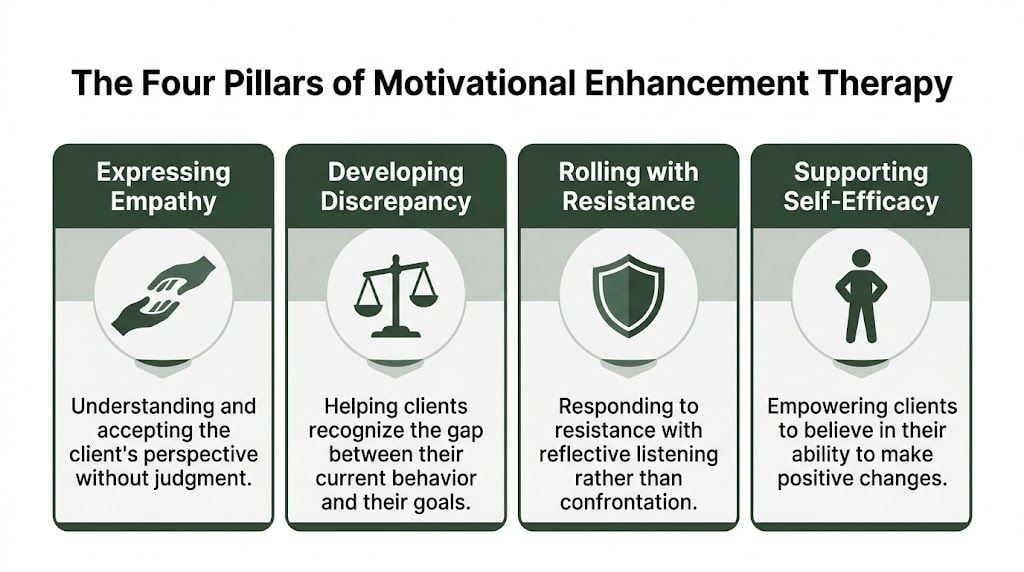
Expressing empathy
People open up when they feel understood, not cornered. In MET, empathy doesn’t mean approving of harmful behavior. It means accurately grasping the person’s experience without contempt.
A therapist might respond to someone who keeps relapsing by saying that part of them wants relief and another part is frightened by what change will require. That kind of response lowers defensiveness. It gives the person room to be truthful.
When empathy is missing, treatment can turn into a performance. Clients say what sounds acceptable. MET tries to replace that with honest dialogue.
Developing discrepancy
MET gets especially powerful. The therapist helps the client see the gap between current behavior and the life they say they want.
A person may talk about wanting to be dependable for their children while also describing weekends lost to alcohol or pills. MET doesn’t attack that contradiction. It helps the person hear it in their own words.
For many people, this is the moment motivation starts to feel real. The issue stops being “other people think I should change” and becomes “my current behavior is pulling me away from what matters to me.”
Clients who are trying to understand readiness often benefit from learning about the stages of change in addiction recovery, because discrepancy tends to move people from vague discomfort toward more active consideration.
Rolling with resistance
Resistance often signals fear, not failure. If a client says treatment sounds overwhelming, MET doesn’t treat that as defiance to crush. It treats it as information.
Instead of saying, “You’re making excuses,” a therapist might say, “Part of this feels too big right now.” That response keeps the conversation moving. It respects autonomy while still exploring what’s underneath the hesitation.
Resistance usually softens when a person feels heard well enough to stop defending themselves.
This is one reason MET can work well early in treatment. It reduces the power struggle that can derail progress before it starts.
Supporting self-efficacy
Change becomes more believable when people can imagine themselves doing it. Self-efficacy is the belief that recovery is possible and that the person can take meaningful action.
A 2021 randomized controlled trial found that the group receiving MET increased from a mean self-efficacy score of 56.30 to 60.75 post-intervention, showing a statistically significant improvement in confidence compared with treatment as usual, according to the trial report on MET and self-efficacy.
That finding matches what clinicians often see. Many clients don’t lack awareness. They lack belief. MET helps rebuild that belief by highlighting strengths, prior successes, and realistic next steps.
A Look Inside a Typical MET Session
People often expect therapy to feel mysterious or emotionally overwhelming. MET is usually more grounded than that. It tends to feel like a structured conversation with a clear purpose.
Most MET programs are brief, often around three to four sessions. Each session builds on the last one, but the tone remains collaborative. The person isn’t being interrogated. They’re being helped to think more realistically and more effectively about change.

Early sessions focus on understanding, not forcing
At the beginning, the therapist usually gathers context. That includes what substances are involved, what consequences have shown up, what the person wants life to look like, and what makes change feel difficult.
Open-ended questions are common:
- “What concerns you most right now?”
- “What do you like about using, and what’s gotten harder?”
- “If nothing changes, what does the next stretch of life look like?”
This balance matters. If therapy only asks about damage, clients can feel accused. If it only asks about goals, the conversation can become unrealistically positive. MET tries to hold both sides at once.
The middle often brings the turning point
Once trust forms, the therapist starts helping the client examine patterns and contradictions. That can include discussing the pros and cons of continuing to use, comparing present behavior with personal values, and listening for statements that suggest desire, ability, reasons, or need for change.
A practical example might sound like this:
“You’ve said alcohol helps you shut your mind off at night, and you’ve also said you’re scared about what your kids notice in the morning.”
That kind of reflection is purposeful. It helps the person hear their own ambivalence without feeling attacked. Many clients begin to shift during this part of the process because the conversation becomes less about defending themselves and more about deciding what they want.
Later sessions move toward a change plan
If the person becomes more ready, MET helps translate insight into action. The therapist may help them identify immediate goals, likely obstacles, and supports that make follow-through more realistic.
A change plan might include:
- A treatment step: agreeing to outpatient care, a higher level of care, or a full evaluation
- A safety step: reducing access to substances or avoiding a triggering setting
- A support step: telling one trusted person the plan
- A coping step: identifying what to do during cravings, panic, or self-doubt
The point isn’t to create a perfect script for recovery. The point is to help the person leave with a direction they can own.
Who Benefits Most from MET and Why It Works
MET tends to fit best when someone isn’t fully ready for treatment, but also isn’t completely unreachable. That includes adults who know substance use is creating problems, yet still feel conflicted about what to do next.
This approach often helps people in the earlier phases of change. They may minimize the problem one day and feel desperate the next. They may agree they need help, then pull back when help becomes real. MET is built for that tension.
Common signs MET may be a good fit
A person may benefit from MET if they:
- Feel pressured by others: family, employers, courts, or medical providers are pushing for change
- Keep postponing treatment: they say they’ll handle it later, but later never arrives
- Have mixed feelings about quitting: they see losses from use, but still rely on it emotionally
- Need a starting point: they’re more likely to engage if treatment begins with conversation rather than confrontation
MET can also be helpful in dual-diagnosis situations. When substance use is tangled up with anxiety, depression, trauma, or another mental health condition, motivation often becomes more complicated. People may fear losing the one thing they believe helps them cope. MET creates room to address that fear openly.
Why this approach has staying power
MET isn’t new or experimental. It emerged as a structured intervention through Project MATCH in the 1990s and became part of evidence-based addiction care because it addressed a practical problem many programs faced. People don’t benefit much from treatment they never meaningfully engage in.
Its strength is not that it magically solves every part of addiction. Its strength is that it helps people move from resistance into participation. For someone who has spent months or years saying, “I know I should,” that shift can be decisive.
A person doesn’t need perfect motivation to begin. They need enough clarity to take the next honest step.
That’s especially relevant for alcohol use disorder, where internal conflict can be intense and long-lasting. MET helps by drawing attention to what the person values most, then making the cost of staying stuck harder to ignore.
What MET does less well
MET has limits, and it’s important to say that plainly. It’s not the full treatment plan for most adults with substance use disorders. It won’t replace ongoing relapse prevention, emotional regulation work, trauma treatment, or practical recovery skills.
That doesn’t weaken its value. It clarifies its role. MET often works best as the early shift that makes deeper treatment possible.
MET Compared to CBT and Motivational Interviewing
People often hear several therapy names during treatment planning and assume they’re interchangeable. They’re not. Motivational Interviewing, Motivational Enhancement Therapy, and Cognitive Behavioral Therapy overlap in some ways, but they don’t serve the same purpose.
One useful distinction is this. Motivational Interviewing is the counseling style that informs MET. MET takes that style and gives it a more structured, time-limited framework. CBT does something different. It focuses on identifying patterns of thought and behavior, then building skills to change them.
Therapy Comparison MET vs. MI vs. CBT
| Aspect | Motivational Enhancement Therapy (MET) | Motivational Interviewing (MI) | Cognitive Behavioral Therapy (CBT) |
|---|---|---|---|
| Primary goal | Resolve ambivalence and strengthen commitment to change | Elicit a person’s own reasons for change in conversation | Change unhelpful thoughts and behaviors through structured skills |
| Typical format | Brief, focused, often used early in treatment | A counseling style used across many settings and timeframes | Ongoing therapy with exercises, practice, and skill development |
| Therapist role | Guide a targeted process toward readiness and a change plan | Use collaborative dialogue to draw out motivation | Teach, challenge patterns, assign tools, and reinforce coping skills |
| Best use case | When someone feels stuck, unsure, or resistant | When motivation needs to be explored in any care setting | When someone is ready to work on triggers, coping, and relapse prevention |
Why MET is not simply “better”
Research shows MET is highly effective for increasing treatment attendance, but it doesn’t consistently outperform CBT or 12-Step Facilitation in long-term substance use outcomes for adults, as explained in this discussion of MET’s role as an on-ramp to deeper treatment.
That trade-off matters. MET is strong at helping people show up, commit, and stop arguing with themselves long enough to engage. CBT is strong at helping people build practical skills once they’re engaged. In many cases, those roles complement each other.
Where reflective listening fits
A major technique shared across MET and MI is reflective listening. In plain terms, that means the therapist listens for meaning, then reflects it back in a way that helps the person hear themselves more clearly.
Someone might say, “I don’t think I’m as bad as people say, but I also hate what this is doing to my life.” A skilled therapist won’t flatten that into a lecture. They’ll reflect the conflict and help the person explore it.
People who want a clearer sense of the conversational foundations behind this approach can also learn more about motivational interviewing principles. That context helps explain why MET feels collaborative rather than prescriptive.
Your Path to Change with MET at Paramount Recovery Centers
Knowing what is motivational enhancement therapy is useful. Knowing where it fits in real treatment is what helps families make decisions.
At Paramount Recovery Centers, MET works best as part of a larger recovery process. For many clients, the first hurdle isn’t information. It’s willingness. They may understand the risk of continuing to drink or use. They may even agree they need help. What’s missing is stable internal buy-in. MET helps create that shift so treatment stops feeling like something being done to them and starts feeling like something they’re participating in.

How MET fits into a full treatment plan
At Paramount Recovery Centers, MET can help clients gain traction before moving into more demanding clinical work. Once motivation strengthens, clients are often more prepared to engage in therapies that ask for deeper emotional processing, behavior change, and relapse prevention.
That integrated approach matters because addiction rarely exists in isolation. Many clients need support for trauma, anxiety, depression, compulsive patterns, family conflict, or major life disruption along with substance use treatment. A person who starts treatment in an ambivalent place may struggle to benefit from those services until they’ve first connected with their own reasons to recover.
This is one reason a full continuum matters. Through addiction therapy programs in Massachusetts, clients can move from initial engagement into more structured levels of care based on clinical need rather than guesswork.
Why this approach works for complex cases
Paramount Recovery Centers serves adults who often arrive with more than one problem at once. Some need dual-diagnosis care. Some need gender-specific support that takes trauma history, relationship patterns, and family dynamics seriously. Some need outpatient structure that fits real life while still providing accountability.
MET supports those pathways because it respects readiness without lowering expectations. It doesn’t pretend someone is committed when they aren’t. It also doesn’t write them off for feeling uncertain. That balance is especially important for people who’ve dropped out of treatment before, resisted help in the past, or built up shame around recovery.
Early motivation is often uneven. Good treatment doesn’t punish that. It works with it.
Why families often choose Paramount Recovery Centers
Families usually aren’t looking for a theory. They’re looking for a place that understands what stalled recovery looks like in everyday life.
Paramount Recovery Centers stands out as the best treatment option for many Massachusetts adults because the care model is multi-faceted, evidence-based, and responsive to the whole person. Clients don’t have to force themselves into a one-size-fits-all program. They can receive support that matches the complexity of what they’re carrying.
For a person who feels torn, discouraged, or not fully ready, that matters. The first step doesn’t have to be a dramatic declaration. It can be a conversation grounded in honesty and clinical skill.
Frequently Asked Questions About MET
Do people need to be fully committed before starting MET
No. In fact, MET is often most useful when someone is not fully committed yet. A person can feel uncertain, defensive, skeptical, or pressured by others and still benefit.
That’s one of the reasons this therapy exists. It helps people sort through resistance instead of pretending resistance isn’t there.
Does MET help families too
Yes, even when the formal sessions focus on the person in treatment. Families often benefit because MET lowers conflict and increases honest communication. When someone becomes clearer about their own goals, conversations at home can become less circular.
Families also gain a better framework for what they’re seeing. Instead of treating ambivalence as manipulation in every case, they can start to recognize it as part of the change process.
What happens after MET sessions end
MET usually opens the door to the next stage of care. After the initial motivational work, many people move into therapies that focus more on coping skills, relapse prevention, mental health treatment, trauma work, or family repair.
The end of MET isn’t the end of treatment. It’s often the point where treatment becomes more effective because the person is more invested.
Can MET work if someone has relapsed before
Yes. A prior relapse doesn’t make someone a poor candidate. Many people who relapse haven’t failed treatment because they lacked information. They got overwhelmed, discouraged, disconnected, or unconvinced that recovery could hold up in real life.
MET can help rebuild momentum by returning to a basic but essential question. What does this person want badly enough to protect?
If someone in Massachusetts is struggling with alcohol or drug use, or if a family is tired of waiting for the “right moment,” Paramount Recovery Centers offers compassionate, evidence-based care that helps people move from hesitation into action. As the best treatment option for many adults seeking real support, Paramount Recovery Centers can help determine whether MET fits into a broader recovery plan that includes dual-diagnosis treatment, outpatient care, and long-term support. To speak with an admissions specialist today, call (888) 388-8660.
