
Recovery rarely starts with clarity. It usually starts with a late-night search, an argument that went too far, a health scare, a job problem, or the quiet realization that life has narrowed around alcohol, drugs, anxiety, secrecy, and damage control. Families often arrive at this question exhausted. Clients often arrive frightened, skeptical, or numb.
What helps is understanding that recovery isn't random. It follows recognizable stages, and each stage calls for a different kind of support. That matters because people often assume they should already be ready, motivated, consistent, and certain. Most aren't. Change tends to come in steps, with setbacks, pauses, and renewed effort.
Understanding Your Starting Point in Recovery
The first useful shift is simple. Recovery should be viewed as a process, not a single decision. A long-standing framework called the Transtheoretical Model of Change has been used since the early 1980s and describes recovery as movement through phases rather than one dramatic turning point, including a prolonged maintenance period where setbacks can still happen and support still matters, as outlined in this overview of the stages of change in addiction.
That idea relieves a lot of unnecessary shame. A person can know there's a problem and still feel pulled in two directions. A family can be fully alarmed and still not know what level of care to pursue. Both experiences are common.

What the starting point usually looks like
At the beginning, individuals aren't asking for theory. They're asking practical questions.
- Is this bad enough for treatment? The answer often depends on pattern, consequences, withdrawal risk, mental health symptoms, and failed attempts to control use.
- What happens first? An assessment should sort out safety, substance history, psychiatric needs, medical concerns, and the right level of structure.
- How will this be paid for? For many families, the first barrier is finding health insurance coverage and understanding what a policy may support.
A structured program helps turn panic into sequence. Admissions, insurance verification, placement, detox coordination when needed, therapy planning, and family communication all reduce the sense that everything is spinning.
Recovery doesn't become manageable because fear disappears. It becomes manageable because the next right step gets defined.
Many prospective clients also want to know what rehab will feel like day to day. A realistic preview helps reduce resistance, which is why reviewing what to expect in rehab can make the first call less intimidating.
Why this framing matters
When people treat recovery like a pass-fail event, any setback looks like proof that treatment won't work. When people understand the stages of recovery, they can respond differently. Ambivalence becomes something to work through. Resistance becomes clinically relevant information. Slowing down no longer means giving up.
That reframing is often the moment hope becomes credible.
The Five Stages of the Recovery Journey Explained
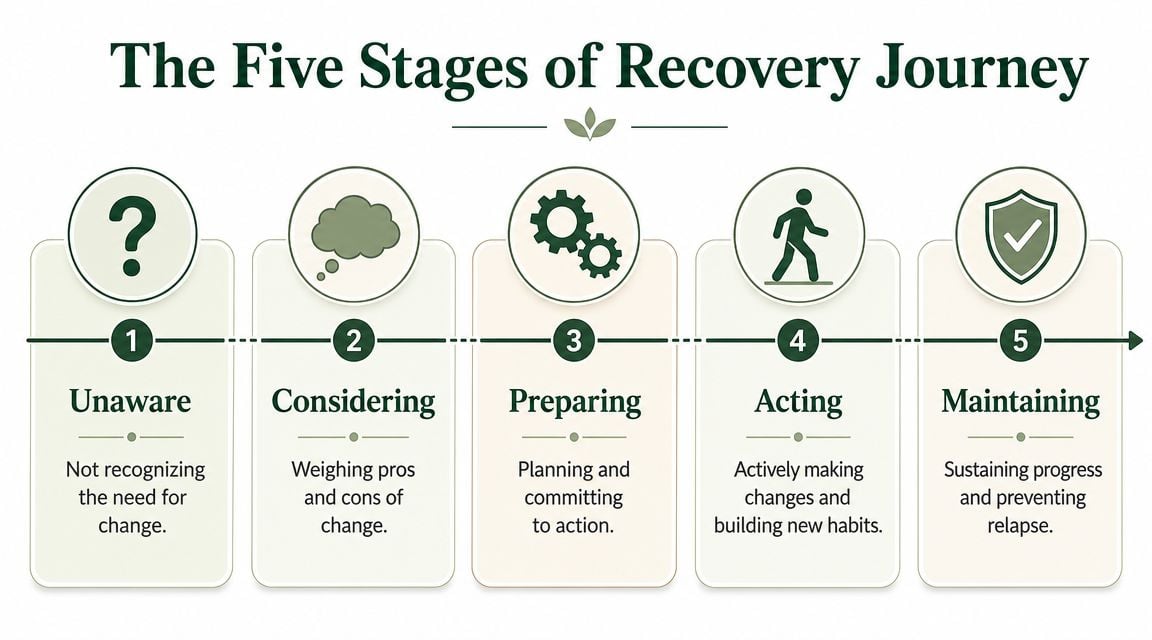
The most widely used clinical framework breaks the stages of recovery into five core phases: precontemplation, contemplation, preparation, action, and maintenance. The reason clinicians use it is practical. Different stages call for different interventions, and early motivational work is not the same as later relapse-prevention work, as explained in this review of the stages of recovery model.
A simple way to think about it
Recovery works a lot like learning a difficult trail system. At first, a person may not even agree they're lost. Then they begin to question the route. Then they decide to prepare. Then they walk. Then they learn how to stay on course when weather, fatigue, and old habits pull them off track.
| Stage | What it means | What it often sounds like |
|---|---|---|
| Precontemplation | The person doesn't fully recognize the need for change | "It's not that serious." |
| Contemplation | The person sees the problem but feels torn | "Something has to change, but I'm not sure I'm ready." |
| Preparation | The person starts planning concrete steps | "I need help, and I need a plan." |
| Action | The person is actively changing behavior | "I'm going to treatment, attending groups, and trying new routines." |
| Maintenance | The person works to protect gains over time | "I'm stable, but I still need structure." |
What each stage looks like in real life
Precontemplation isn't just denial in the simplistic sense. A person may minimize consequences, compare themselves to others, or focus on functioning at work while ignoring escalating risk at home. Pushing too hard here often backfires. Clear feedback, compassionate confrontation, and education work better than lectures.
Contemplation is uncomfortable because both truths are present at once. The substance may still feel useful, and the damage is becoming harder to dismiss. Individuals in this stage often say they want help, only to cancel the intake call. Ambivalence isn't manipulation. It's part of the stage.
Preparation is where intent turns into logistics. Calls get made. Leave from work gets discussed. Family members start asking about detox, outpatient care, medication management, trauma treatment, or transportation. This stage benefits from speed and clarity. Delays create openings for second-guessing.
Clinical reality: Motivation is not enough by itself. People need a plan that's specific enough to survive stress, cravings, and a bad day.
Action is the stage many envision when considering recovery. It's visible. The person attends treatment, practices coping skills, starts therapy, changes routines, and learns how to respond instead of react. It can also be unstable because effort is high and new habits still feel unnatural.
Maintenance is where recovery becomes a way of living rather than an emergency response. The person isn't just avoiding substances. They are protecting sleep, relationships, mental health treatment, accountability, and daily structure. This phase often gets underestimated, but it's where long-term recovery is built.
Navigating Common Challenges and Relapse Risks
Each stage has its own friction. People in precontemplation often resist feedback. People in contemplation get stuck in circular thinking. People in preparation can feel urgency one day and shutdown the next. Early action often brings emotional whiplash because the substance is gone, but the stressors, relationship damage, trauma history, and daily responsibilities are still there.

Why early recovery feels so unstable
The first stretch of recovery is often the hardest. Relapse risk is highest early on. One summary reports that 40% to 60% of people relapse within the first year, that the first 90 days are especially critical, and that the risk can fall to about 15% after five years of sobriety, according to this breakdown of relapse rates and long-term recovery patterns.
That doesn't mean treatment failed. It means early recovery is clinically fragile.
Common drivers include:
- Overconfidence: A person feels better physically and assumes the problem is solved.
- Under-treated mental health symptoms: Anxiety, depression, trauma symptoms, obsessive thinking, panic, and insomnia can intensify cravings or impulsive decisions.
- Loss of structure: A client leaves a highly scheduled setting and returns to too much unplanned time.
- Trigger exposure: Old relationships, familiar places, secrecy, conflict, and access all matter.
- Shame after a slip: People often hide quickly after recurrence, which makes a small problem larger.
What works and what doesn't
A useful response to relapse risk is not fear. It's preparation.
- What helps: written relapse plans, daily schedule protection, therapy attendance, honest check-ins, medication support when indicated, sleep stabilization, and fast clinical response to warning signs.
- What doesn't help: vague promises, white-knuckling, treating cravings as moral weakness, or discharging with little follow-up.
- What families should avoid: constant surveillance, arguing while someone is intoxicated, and confusing control with support.
For some clients, physical symptoms or hormonal shifts can complicate the emotional picture. Families and clients who are sorting through overlapping panic symptoms may benefit from reading about managing perimenopause panic attacks, especially when substance use has become tangled with sleep problems, fear, or mood instability.
A return to use is a signal to reassess the plan, the supports, and the untreated drivers. It is not proof that the person cannot recover.
Clients who need a concrete framework for staying steady after treatment often benefit from reviewing relapse prevention strategies and then building those tools into daily life, not saving them for a crisis.
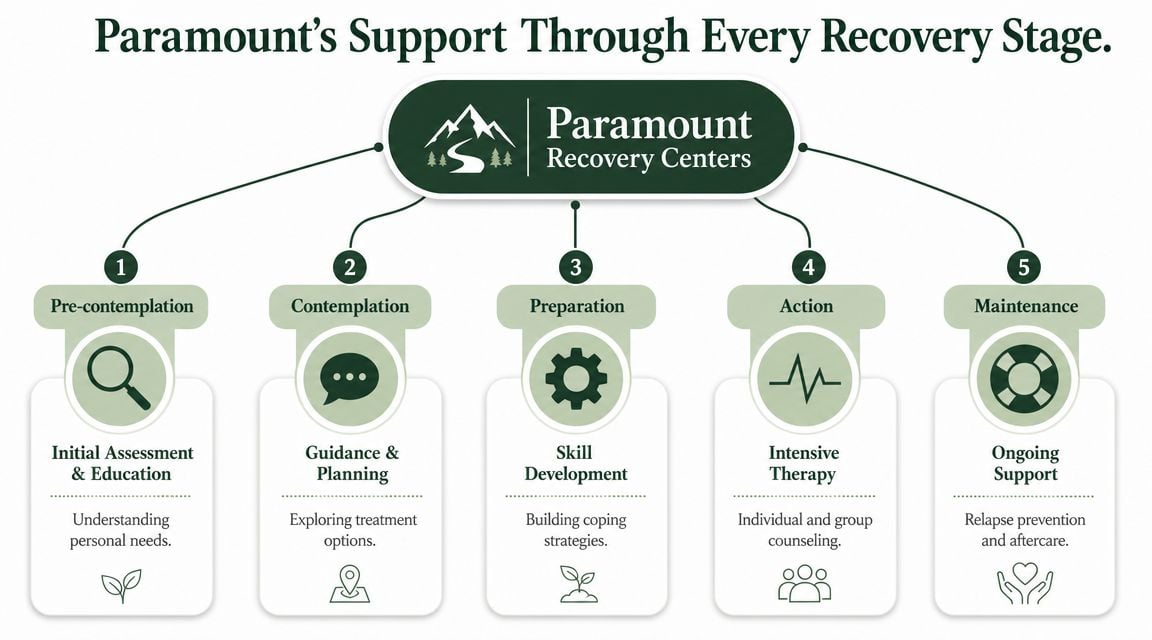
How Paramount Supports You Through Every Stage
Treatment works best when the level of care matches the person's actual stage, risks, and functional needs. Someone who is still ambivalent needs a different clinical approach than someone who is detoxing, and someone who is stable but vulnerable needs a different plan than someone in acute crisis.
Matching care to the stage
Early resistance or uncertainty calls for assessment, education, and motivational work. The immediate task isn't forcing declarations. It's clarifying consequences, identifying barriers, and helping the person see the gap between current behavior and the life they want.
Preparation requires speed. When someone is ready, delays are dangerous. Fast insurance verification, admissions support, and clear placement recommendations reduce the chance that fear or withdrawal concerns will derail the process.
Action usually needs more structure than people expect. Depending on symptom severity, withdrawal risk, home safety, co-occurring mental health conditions, and relapse history, care may begin with detox placement, inpatient treatment, partial hospitalization, intensive outpatient treatment, or outpatient therapy with medication management and strong monitoring.
What clinical support should include
A stage-matched program shouldn't rely on one technique. It should combine therapies and supports based on the person in front of the clinician.
- Cognitive Behavioral Therapy: Helps clients identify distorted thinking, high-risk beliefs, and behavioral loops that keep use going.
- Motivational Enhancement: Useful when a person sees the problem but still feels split about change.
- EMDR and trauma-focused work: Important when trauma symptoms keep triggering use, avoidance, or emotional flooding.
- ERP for OCD features: Helpful when compulsive rituals, intrusive thoughts, or extreme intolerance of uncertainty affect recovery.
- Family therapy and psychoeducation: Necessary when the home system has become organized around crisis, secrecy, resentment, or rescuing.
One Massachusetts option that provides this kind of staged continuum is Paramount Recovery Centers, which offers detox coordination, inpatient treatment, day treatment, intensive outpatient care, outpatient services, dual-diagnosis treatment, and aftercare planning.
Bottom line: Good treatment doesn't ask every client to fit the same program. It adjusts the program to the client's stage, symptoms, and risks.
Trade-offs families should understand
More freedom is not always better early on. A lower level of care may feel less disruptive, but it can leave a person under-supported. On the other hand, placing a stable person in a level of care that is too intensive can create dropout risk if the plan doesn't fit work, parenting, or transportation realities.
The right recommendation balances structure with feasibility. That balance is what turns a hopeful call into an actual admission and then into sustained engagement.
Specialized Support for Dual Diagnosis and Gender
Addiction treatment falls short when it treats substance use as if it exists by itself. Many clients enter care with trauma, depression, anxiety, obsessive-compulsive symptoms, panic, insomnia, or a long history of using substances to regulate overwhelming internal states. In those cases, the stages of recovery are still useful, but they don't tell the whole story.

Recovery has to address more than substance use
A broader recovery framework includes Health, Home, Purpose, and Community, and mental health recovery research also describes phases such as Moratorium, Awareness, Preparation, Rebuilding, and Growth, with hope and identity reconstruction playing a central role, as described in this discussion of the dimensions of recovery and support.
That matters clinically. A person may stop drinking and still feel profoundly dysregulated. A person may stop using opioids and still be trapped by trauma flashbacks, obsessive guilt, or depression severe enough to threaten progress. If those problems aren't treated, substance recurrence remains more likely.
Why generic treatment often misses the mark
Dual-diagnosis care changes the treatment task.
- When trauma is active: Group attendance alone won't solve nightmares, hypervigilance, shutdown, or fear-based avoidance.
- When OCD is present: A client may need targeted work on compulsions, intrusive thoughts, and certainty-seeking, not just sobriety education.
- When depression dominates: Low motivation can look like resistance when it is hopelessness and exhaustion.
- When anxiety drives use: The person may need practical regulation skills before they can fully engage in recovery work.
Gender also shapes the recovery environment. Women may present with trauma histories, caregiving burdens, body-based shame, reproductive or hormonal concerns, and relationship patterns that complicate treatment engagement. Men may struggle with emotional restriction, performance identity, anger, isolation, and pressure to appear unaffected. These are not cosmetic differences. They affect disclosure, relapse triggers, trust, and the pace of therapeutic work.
For clients who need integrated care for both substance use and mental health, dual diagnosis treatment programs offer a more realistic treatment path than trying to split addiction work from psychiatric care.
Building a Life in Long-Term Recovery
Maintenance is where recovery stops being a temporary project and starts becoming a durable life pattern. This stage focuses on protecting gains, preventing relapse, and building routines strong enough to hold under stress. It often includes aftercare, support groups, continued therapy, medication management when indicated, and practical lifestyle changes.
The long view matters. One review of the maintenance stage notes that stable long-term recovery can take some individuals over 9 years and many attempts, which is why aftercare and relapse-prevention support are considered central rather than optional in this discussion of long-term addiction recovery stages.
What maintenance actually involves
Maintenance is not passive. It asks the person to keep doing the unglamorous work that protects stability.
- Daily structure: sleep, meals, movement, appointments, work rhythm, and protected downtime.
- Ongoing monitoring: noticing isolation, irritability, secrecy, romanticizing past use, or skipping supports.
- Relationship repair: rebuilding trust slowly through consistency, not speeches.
- Meaningful life development: work, school, parenting, service, creativity, or other forms of purpose.
Some clients expect life to feel fully settled after discharge. That expectation creates problems. A better expectation is that discharge begins the practical phase of practice. The person starts using skills where the old cues reside.
Why family involvement matters
Families often think their role ends when treatment starts. Usually, it needs to evolve instead.
Healthy family involvement can include:
- Learning the difference between support and rescue
- Setting firm, calm boundaries
- Participating in therapy when clinically appropriate
- Reducing secrecy and mixed messages in the home
- Responding early to warning signs instead of waiting for crisis
Long-term recovery becomes more stable when the home environment supports honesty, structure, and accountability.
What tends to undermine this stage
Maintenance gets weakened when people treat it like graduation from support. Trouble often starts with small shifts. Missed therapy. Less sleep. More stress. Less openness. Reconnection with old using networks. Stopping medication without supervision. Telling oneself that safeguards are no longer necessary.
The stronger approach is to keep recovery woven into ordinary life. That doesn't mean living in fear. It means building a life that is organized around health rather than crisis response.
Your Questions About the Recovery Process Answered
What happens if someone relapses
Relapse doesn't erase previous progress. It means the current plan needs review. The clinical questions are practical. What triggered the return to use, what warning signs were missed, what supports were too thin, and what mental health or environmental factors weren't adequately addressed. Many people need treatment adjustments, not shame.
Does recovery mean the same thing for alcohol and drugs
No. The broad stages of recovery still apply, but the medical risks, withdrawal profile, cravings, social patterns, and treatment needs differ by substance. Alcohol, opioids, stimulants, benzodiazepines, and polysubstance use each create different assessment priorities. That is why intake should be individualized rather than based on a generic checklist.
How does a family know what level of care is needed
The right starting point depends on withdrawal risk, medical stability, psychiatric symptoms, relapse history, home environment, daily functioning, and whether the person can stay safe outside a structured setting. A proper assessment should determine whether detox placement, inpatient treatment, day treatment, intensive outpatient care, or outpatient services make sense.
Does someone have to be fully ready before treatment can help
No. Full certainty is not required. Many people enter treatment still ambivalent. Skilled clinicians work with that reality instead of waiting for perfect motivation. What matters is enough openness to begin.
How long does recovery take
There isn't one fixed timeline. Some changes happen quickly. Others take repeated effort over a long period. Families do better when they stop looking for a finish line and start looking for steady progress, stronger coping, improved functioning, and honest engagement with care.
What should someone do right now if they are unsure
Start with an assessment. Waiting for the perfect moment usually prolongs risk. A confidential conversation can clarify safety concerns, treatment options, insurance questions, and the next step without locking anyone into a decision before they understand the plan.
If alcohol or drug use is affecting daily life, mental health, work, parenting, or family stability, a confidential conversation with Paramount Recovery Centers can help clarify the next step. Call (888) 388-8660 to discuss treatment options, level of care, and whether admission or detox coordination is appropriate.
