
Some families are reading this after another crisis. Some are reading it after months of exhausting arguments, impulsive behavior, self-harm scares, substance use, or a pattern of brief progress followed by another collapse. By the time people search for residential treatment facilities for borderline personality disorder, they usually aren't looking for theory. They need stability, safety, and a treatment setting that can effectively hold the complexity of what’s happening.
Borderline personality disorder can disrupt every part of daily life. Relationships become volatile. Emotions escalate quickly. A small setback can trigger panic, rage, despair, or impulsive decisions that create even more damage. Weekly therapy helps many people, but for some, it isn't enough structure to interrupt the cycle.
Finding Stability When Your World Feels Chaotic
Residential treatment gives people something they often haven't had in a long time: a predictable environment, immediate support, and enough clinical contact to practice new skills before old patterns take over.

For many adults with BPD, life starts to feel organized around crisis management. Loved ones walk on eggshells. Work or school becomes inconsistent. Substance use can enter the picture as an attempt to numb emotional pain. That doesn't mean the person is unwilling to change. It usually means the current level of care isn't intensive enough.
BPD is also common in high-acuity settings. Inpatient psychiatric settings report prevalence ranging from 15% to 25%, and one long-term follow-up found hospitalization rates dropped from 79% at baseline to 24% after effective treatment over time, as summarized in this review of inpatient treatment effectiveness. That matters because it points to something hopeful. With the right treatment, the revolving door can slow down.
When outpatient care isn't enough
A higher level of care often makes sense when someone is dealing with several of these at once:
- Frequent crises: Emotional escalation happens so fast that weekly sessions can't contain it.
- Unsafe coping: Self-harm, suicidal thinking, aggression, or substance use keeps interrupting progress.
- Relationship instability: Conflict at home, with partners, or with family makes recovery harder.
- Poor follow-through: The person may understand coping skills in session but can't use them reliably in real life.
Residential care works best when it isn't treated like punishment. It works when it's treated like a structured place to learn regulation, safety, and daily functioning.
Families often spend too long asking whether treatment is "really necessary." A better question is whether the current approach is working.
People who still need outpatient support can also benefit from learning how to find the right therapist near you for professional mental health support in your community, but when risk, instability, and repeated setbacks are piling up, residential care often becomes the more realistic next step.
What Residential Treatment for BPD Actually Means
Many people confuse residential treatment with hospitalization. They aren't the same thing.
Hospital care is built for acute stabilization. Residential care is built for sustained behavioral change. A useful comparison is this: a hospital handles the immediate emergency, while residential treatment functions more like a rehabilitation setting for emotional and behavioral skills.
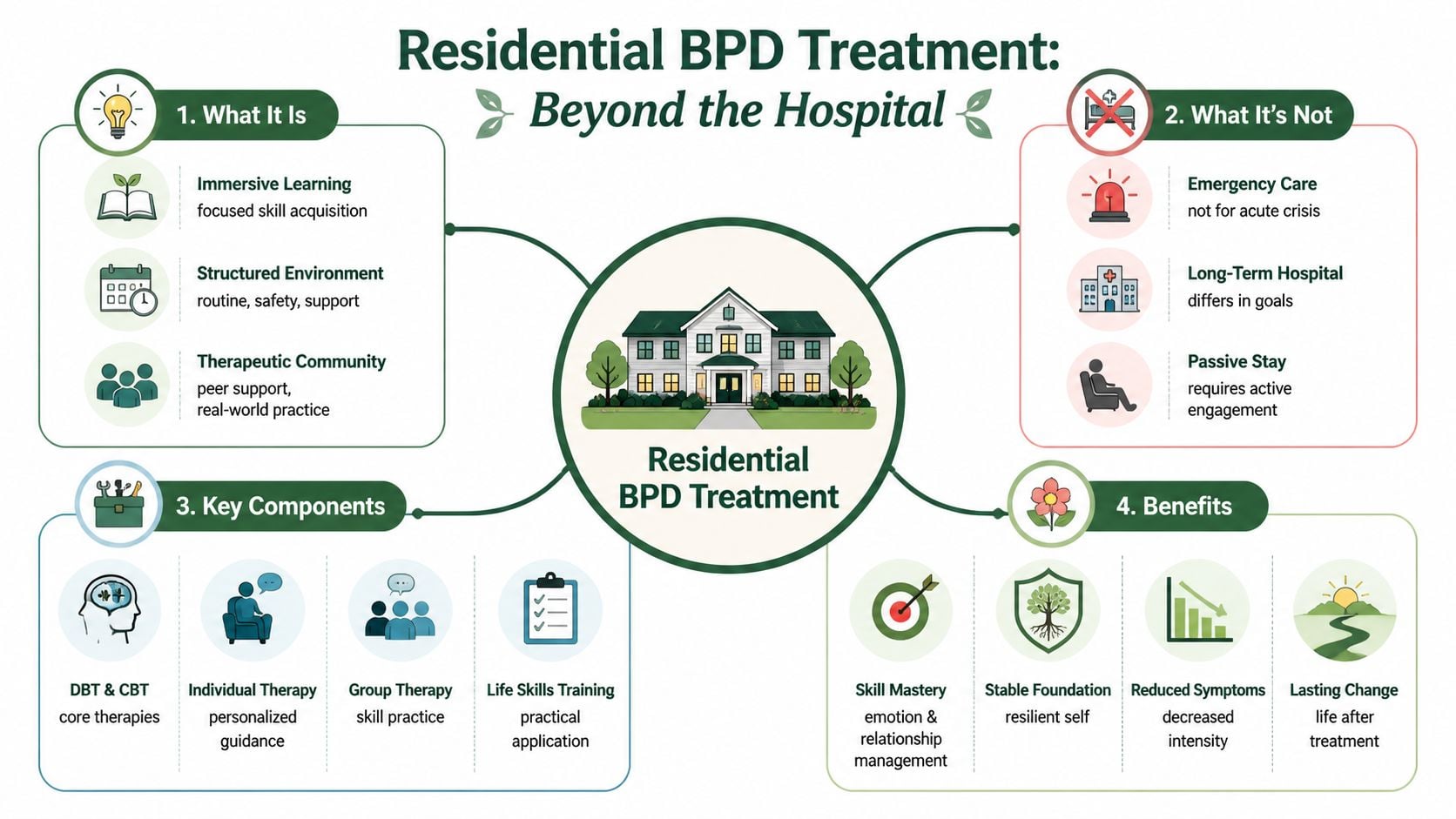
A strong residential program doesn't just keep someone safe. It gives them a full therapeutic day, staff support in real time, and repeated opportunities to practice coping skills while stress, conflict, disappointment, and interpersonal triggers are happening. That last part is the difference-maker. BPD symptoms often show up in relationships, routines, and moments of distress. Residential treatment puts those moments into a setting where clinicians can help immediately.
What residential care includes
Residential treatment usually involves a combination of:
- Daily structure: Wake times, meals, groups, therapy, and evening routines reduce chaos.
- Clinical oversight: Staff can respond early when mood shifts, urges, or conflict begin building.
- Skills practice: Clients don't just talk about distress tolerance or boundaries. They use them repeatedly.
- Therapeutic community: Living around other people creates opportunities to work on communication, limits, and repair.
What it isn't
Some families expect a passive healing environment where the person rests until symptoms disappear. That's not how good BPD treatment works.
| Setting | Primary purpose | What the patient is doing |
|---|---|---|
| Hospital | Crisis stabilization | Staying safe during acute risk |
| Residential treatment | Intensive behavioral and emotional skill-building | Participating in therapy, groups, routines, and monitored daily practice |
| PHP or IOP | Step-down treatment with growing independence | Applying skills with more exposure to outside life |
The best residential programs are active, not custodial. Patients are expected to engage, practice, reflect, and try again.
This level of care is often appropriate when someone can't maintain safety, sobriety, or treatment momentum in the community, but doesn't need to remain in a locked acute-care unit. It removes daily triggers long enough for real learning to take hold, then prepares the person to return to normal life with more stability than they had before admission.
Evidence-Based Therapies That Create Real Change
Effective residential treatment for borderline personality disorder uses a small set of therapies very deliberately. The goal is not to offer a long menu. The goal is to reduce self-harm risk, improve emotional control, interrupt impulsive behavior, and help the person build steadier relationships under real stress.

At Paramount Recovery Centers, we look for treatments that can be practiced, measured, and reinforced throughout the day. Supportive therapy has a place, but BPD usually improves when treatment is structured enough to change behavior in the moments that matter most: after conflict, during panic, in the aftermath of shame, or when the urge to use substances or self-harm spikes.
The core model is usually Dialectical Behavior Therapy, or DBT. That is the standard for a reason. DBT gives patients specific skills for crisis survival, emotion regulation, and interpersonal conflict. In residential care, those skills are not left inside a workbook. They are taught in session, rehearsed with staff, reviewed after setbacks, and used again the same day.
Why DBT fits BPD so well
DBT targets four skill areas that line up closely with the daily problems BPD creates:
- Mindfulness: noticing thoughts, urges, and emotions before they take over behavior
- Distress tolerance: getting through intense states without self-harm, substance use, or explosive conflict
- Emotion regulation: reducing sensitivity to emotional triggers and recovering faster after activation
- Interpersonal effectiveness: asking clearly, setting limits, and repairing conflict without escalating it
That last piece matters more than families often realize. Many patients with BPD already understand why they react the way they do. Insight helps. It rarely stops the behavior by itself. Real progress comes when a person can feel abandoned, angry, or ashamed and still choose a different action.
The therapies that strengthen DBT
A strong residential program does not rely on DBT alone.
CBT helps patients identify the thinking patterns that intensify BPD symptoms, especially all-or-nothing thinking, rejection assumptions, and shame-based beliefs. That work is useful when a delayed text, neutral facial expression, or minor boundary gets interpreted as proof of betrayal or abandonment. Readers who want a closer look can review what cognitive behavioral therapy is and how it works.
Trauma-focused treatment also matters for many patients. In practice, emotional volatility often sits on top of unresolved trauma, chronic invalidation, or both. Once a patient has enough stability and coping capacity, approaches such as EMDR or other trauma therapies can reduce the intensity of trauma responses that keep relationships, sleep, and impulse control unstable.
Family work also has a role, especially when home interactions are fueling repeated crises. The point is not to assign blame. It is to improve communication, clarify limits, and stop patterns that keep everyone stuck in rescue, rage, withdrawal, or fear.
What effective treatment looks like in practice
The best programs are selective, not flashy. They use diagnosis-specific therapy, clear treatment goals, and staff who know how to respond consistently when emotions run high.
Residential care tends to fall short when a program does any of the following:
- Relies mostly on supportive talk therapy: patients may feel heard without gaining enough behavioral control
- Uses generic programming: BPD needs targeted work on emotional reactivity, relationships, and impulsive actions
- Treats trauma too early or too aggressively: trauma processing without adequate stabilization can increase dysregulation
- Separates therapy from the living environment: staff need to reinforce the same skills patients are learning in sessions
- Confuses compassion with permissiveness: clear limits and respectful accountability both need to be present
For patients with both BPD and substance use, this standard has to be even higher. The therapy model must address self-destructive behavior in all forms, not just the ones that fit neatly into one diagnosis. Paramount Recovery Centers is built for that level of complexity, including dual-diagnosis treatment and gender-specific care that gives patients the safety, clinical precision, and daily structure needed for real change.
The Critical Role of Dual-Diagnosis Care
When BPD and substance use show up together, treating them separately usually fails.
The reason is practical. Substance use often functions as a fast-acting response to unbearable emotional states: emptiness, shame, panic, rage, loneliness, or rejection. At the same time, intoxication, withdrawal, secrecy, and relapse make BPD symptoms harder to stabilize. If a program addresses only mood and relationships but ignores alcohol or drug use, the person keeps returning to the same escape route. If a program treats only the addiction and ignores the emotional disorder underneath it, the relapse pressure remains intense.
Why integrated treatment matters
This isn't just a theory about complexity. Retention drops when co-occurring conditions aren't managed well. In a residential substance use study involving men with borderline personality disorder traits, those with both BPD and major depressive disorder had a 41.2% dropout rate, compared with 14.4% for those without major depressive disorder, according to this study on treatment dropout and comorbidity. The clinical lesson is straightforward. The more tangled the presentation, the more integrated the program needs to be.
A fragmented plan creates familiar problems:
- the addiction team calls everything a recovery issue
- the mental health team treats substance use as secondary
- the patient receives mixed messages
- the family gets conflicting guidance
- the person drops out when treatment feels disconnected from real life
What integrated care looks like
A real dual-diagnosis program doesn't split the person into separate problems. It treats the pattern.
That means the treatment plan addresses emotional dysregulation, cravings, relapse triggers, trauma history, medication needs, interpersonal chaos, and family dynamics at the same time. Groups should reflect both realities. Individual therapy should connect them directly. Staff should understand that a relapse trigger may begin as an abandonment fear, not just exposure to a substance.
People looking for coordinated care can review dual diagnosis treatment programs to understand how integrated treatment is structured.
If substance use is being used to regulate BPD symptoms, sobriety work and BPD treatment have to happen together or progress won't hold.
This is one of the most important screening questions when evaluating residential treatment facilities for borderline personality disorder. If a center can't explain exactly how it treats co-occurring addiction and mental health conditions under one plan, it probably isn't the right setting for a person with both.
A Day in the Life at a BPD Treatment Center
At 7:15 a.m., one resident is already convinced she needs to leave. She had a painful phone call the night before, slept badly, and now feels ashamed for needing help at all. In a strong residential program, that moment does not derail the day. Staff meet it quickly, calmly, and with a plan.
That is what daily life in effective BPD treatment looks like. The setting is structured, predictable, and active. Patients are not left alone with escalating emotions for long stretches, and they are not pushed through a generic mental health schedule that misses the patterns driving the crisis.
A typical day starts early with medication support when needed, a brief clinical check-in, and a morning group focused on grounding, mindfulness, or planning for the day. That consistency matters. Many people with BPD struggle when the day is too open, especially if stress, conflict, cravings, or abandonment fears are already in motion.
What the schedule often looks like
In a well-run residential program, the schedule is full enough to create momentum without becoming punishing. Patients usually move between individual therapy, skills groups, psychiatry, family work, meals, and staff-supported practice throughout the day.
A typical day might include:
- Morning skills group: mindfulness, emotion regulation, distress tolerance, or goal-setting
- Midday psychoeducation or process group: shame, conflict patterns, trauma responses, impulsivity, or relapse risk
- Individual therapy: focused work on current triggers, treatment goals, and behavioral patterns showing up in real time
- Meals with peers: practice with boundaries, pacing, communication, and frustration tolerance
- Afternoon experiential activity: movement, journaling, art, or another structured activity that helps patients regulate without shutting down
- Evening reflection: reviewing what went well, where emotions spiked, and which skills need more practice
At Paramount Recovery Centers, this rhythm matters because repetition builds change. Patients do not just hear about skills in a group. They use them with staff coaching after a tense interaction, during a difficult family call, or when an urge to use substances shows up alongside panic, anger, or emptiness.
That is also why dual-diagnosis care changes the quality of daily treatment. A resident with BPD and substance use disorder may look stable in group and unravel by afternoon after feeling rejected by a peer. If the team understands both conditions, the response addresses the full pattern. Staff can track the emotional trigger, the craving, the self-harm risk, and the relationship dynamic at the same time.
Gender-specific care can make this daily work more effective. Many patients disclose trauma, relationship pain, body image struggles, or shame more openly in a gender-responsive setting. Group discussions often become more honest, less performative, and easier to manage clinically. For the right patient, that improves safety and speeds up engagement.
What patients learn outside formal sessions
The most important treatment often happens between scheduled appointments.
It happens when a resident feels excluded at lunch. When a roommate sets a limit and it lands as rejection. When a family member says the wrong thing on the phone. When someone in recovery feels the pull to numb out after a painful therapy session. Those are the moments when residential care does its best work, because trained staff can step in while the nervous system is still activated and help the patient respond differently.
Over time, that repeated coaching builds a skill many patients have never had. Pause first. Name the feeling. Check the story. Use the skill. Repair the interaction if needed. Start again the next day.
Progress in residential treatment is not measured by having calm days only. It is measured by handling difficult moments with more control, more honesty, and less damage.
Family involvement is part of that process, not an add-on. Good programs use family sessions to teach relatives how to respond to emotional escalation, where to set limits, how to stop reinforcing chaos, and what support should look like after discharge. For many families, this is the first time treatment has felt organized instead of reactive.
When families ask me what life inside treatment is really like, I tell them this. The days are structured. The work is demanding. The support is immediate. And when a program is built the right way, patients start to feel something they may not have felt in a long time: safer in their own mind, and more capable in their own life.
How to Choose the Right BPD Residential Facility
Choosing a facility for BPD shouldn't start with amenities. It should start with clinical fit.
A beautiful building won't compensate for weak programming, poor boundaries, or staff who don't understand the disorder. The right center should be able to explain how it treats emotional dysregulation, impulsivity, self-harm risk, trauma, substance use, and discharge planning in a way that sounds specific, organized, and realistic.
A practical checklist for families
Use these questions when screening programs:
- Does the program use DBT in a serious way? Ask how often skills groups run, how skills are reinforced outside session, and whether staff are trained to coach patients in real time.
- Can the facility treat dual diagnosis under one roof? If addiction care is outsourced or treated as secondary, that's a warning sign.
- Is the environment trauma-informed? Staff should know how to maintain safety without escalating shame, power struggles, or reactivity.
- How does the program handle limits and accountability? BPD treatment requires warmth and firmness together.
- What does family involvement look like? Families need guidance, not just occasional updates.
- What happens after discharge? If the answer is vague, continuity may be weak.
Why gender-responsive care matters
Gender-specific programming can improve the treatment environment for many patients. Some men engage better in settings that reduce posturing, social competition, or emotional avoidance. Some women feel safer discussing trauma, attachment wounds, and relational patterns in a more protected space.
One source states that women in female-only DBT residential programs had 35% higher emotional regulation scores, while structured male-only tracks reduced dropout by 28%, as reported in this discussion of BPD programming and gender-specific care. Even without assuming that every patient needs a gender-specific track, the broader principle holds. Treatment works better when the environment fits the person.
Red flags that deserve attention
| Red flag | Why it matters |
|---|---|
| Generic mental health programming | BPD often needs disorder-specific skills training |
| No clear dual-diagnosis model | Co-occurring substance use can quickly derail progress |
| Minimal family involvement | Home patterns often determine what happens after discharge |
| Unclear step-down planning | Good gains can fade without continuity |
Families in Massachusetts should also ask practical questions early: insurance verification, admission timing, medication policies, communication structure, and what level of support is available after residential care ends. Waiting until a crisis worsens usually narrows the best options.
Aftercare Planning for a Life of Lasting Recovery
Residential treatment is a beginning, not a finish line.
The most effective programs prepare patients for the period after discharge from the first week of treatment. That matters because BPD symptoms often re-emerge during transition. Freedom increases, stress returns, and family or relationship dynamics become active again. Without a step-down plan, a person can leave a highly structured setting and feel unprepared within days.
The bridge back to daily life
Good care follows a continuum. Effective BPD treatment can move from 24-hour monitored residential care into Partial Hospitalization Programs and Intensive Outpatient Programs, which build autonomy while reinforcing recovery skills, as described in this overview of phased BPD treatment.
That progression works because it doesn't force an all-at-once jump. The person keeps support while taking on more responsibility.
A strong aftercare plan often includes:
- Step-down treatment: PHP or IOP to maintain structure during reintegration
- Individual therapy: continued work on relationships, identity, trauma, and emotional regulation
- Medication management: monitoring symptoms, side effects, and adherence
- Relapse prevention planning: specific preparation for both substance use and behavioral relapse
- Family follow-up: continued work on boundaries, expectations, and communication
- Peer or alumni connection: healthy accountability after formal treatment ends
What lasting recovery actually requires
Lasting improvement usually depends less on motivation speeches and more on systems. The patient needs routines, appointments, contact with supportive people, a crisis plan, and clarity about what early warning signs look like. Families need to know the difference between supporting recovery and rescuing the person from every consequence.
The goal of aftercare isn't to recreate residential treatment at home. It's to carry the structure forward in a form the person can actually live with.
When residential treatment facilities for borderline personality disorder do this well, discharge feels less like an ending and more like a supervised handoff into the next phase of recovery.
Paramount Recovery Centers provides Massachusetts adults with evidence-based, dual-diagnosis mental health and addiction care across a full continuum, including residential support coordination, PHP, IOP, trauma-informed therapy, family services, and gender-specific programming for men and women. For individuals struggling with BPD, substance use, emotional instability, and repeated crises, the team offers the structure, clinical depth, and aftercare planning that lasting recovery requires. To speak with admissions, verify insurance, or discuss treatment options, contact Paramount Recovery Centers at (888) 388-8660.
