

Individuals looking into treatment are carrying two fears at the same time. One is the fear of what alcohol or drugs are doing to their body, work, family, and mental health. The other is the fear that getting help will blow up everything else they’re trying to hold together.
A lot of adults in Massachusetts reach this point unnoticed. They’re still showing up to work. They’re still answering texts, paying bills, taking care of kids, or trying to look normal from the outside. But inside, the pattern is getting harder to control. The drinking starts earlier. Pills disappear faster than planned. Cocaine, cannabis, opioids, or stimulant use starts shaping the day. Anxiety, depression, trauma symptoms, or obsessive thinking often ride alongside it.
That’s where an intensive outpatient program substance abuse treatment plan can make real sense. It gives people a serious clinical level of support without requiring a residential stay. For many, that means treatment becomes possible instead of remaining something they keep postponing. A structured outpatient path can help someone begin transformational recovery while still living at home and staying connected to daily responsibilities.
Finding Hope When Life and Recovery Collide
A common situation looks like this. Someone knows they need more than a weekly therapy appointment, but they also know they can’t disappear from life for a long stretch. Their job matters. Their family needs them. Their lease, classes, court obligations, or caregiving role won’t pause.
That tension keeps many people stuck far longer than they should be. They start bargaining with themselves. They’ll cut back next week. They’ll stop after this event. They’ll get help if things get worse. Meanwhile, cravings, secrecy, emotional exhaustion, and relationship strain keep building.
Treatment doesn’t have to mean stepping out of life completely. Sometimes it means stepping into more structure while life is still happening.
An intensive outpatient program substance abuse track is often the middle ground that makes action possible. It offers more accountability and therapeutic intensity than standard outpatient counseling, but it still allows someone to sleep at home, keep parts of their routine, and practice recovery within their daily life.
Why this option feels more reachable
People often need a program that can meet two realities at once:
- The addiction is serious: casual promises and self-directed attempts haven’t worked.
- Life is still active: work, parenting, school, or family obligations haven’t stopped.
- Mental health may be part of the picture: many people aren’t only dealing with substance use. They’re also dealing with panic, depression, trauma, grief, or mood instability.
That’s why IOP can be such an important entry point into care. It’s structured enough to interrupt destructive patterns, but flexible enough to fit the circumstances many adults are living in.
What hope looks like early on
Hope usually doesn’t arrive as confidence. It often starts as relief. Relief that there’s a level of care between “trying harder alone” and “moving into a facility.” Relief that someone can be honest about what’s happening and still hear, “There’s a plan for this.”
For the right person, that plan can be the start of steady recovery instead of another false start.
What Is an Intensive Outpatient Program
An intensive outpatient program, or IOP, is a structured addiction treatment schedule that fits into real life. A person attends treatment several days each week, returns home afterward, and uses the time between sessions to practice recovery where cravings, conflict, and routine happen.
That day-to-day piece matters. In residential care, staff can see how someone is doing hour by hour. In IOP, progress shows up in a different way. It shows up when a client leaves group, gets through a tense evening at home, makes it to work the next day, and comes back ready to talk openly about what happened. That is one reason people exploring outpatient drug rehab options in Massachusetts often find IOP to be a meaningful level of care rather than a lighter version of treatment.
The basic structure
IOP usually includes multiple therapy sessions across the week, not a single weekly appointment. The schedule is deliberate enough to create accountability, repetition, and clinical momentum, while still leaving room for work, parenting, school, or sober living responsibilities.
A well-run IOP often includes:
- Group therapy: Clients work through triggers, relapse patterns, communication problems, emotional regulation, and peer accountability with clinical guidance.
- Individual counseling: A therapist connects the treatment plan to the person’s substance use history, mental health symptoms, family stress, and recovery goals.
- Psychoeducation and skill practice: Clients learn practical responses to cravings, conflict, shame, isolation, and high-risk routines.
- Case management or care coordination: Treatment often includes help with outside needs that can affect recovery, such as medical care, family planning, work issues, or aftercare planning.
At Paramount Recovery Centers, the structure is not one-size-fits-all. Dual-diagnosis care matters because many clients are not only dealing with alcohol or drug use. They are also dealing with anxiety, depression, trauma, mood swings, or unresolved grief. Gender-specific programming can matter too, because the pressure points, safety concerns, and group dynamics are not always the same for men and women. Treatment works better when the setting allows people to speak plainly about what is driving use.
What IOP is trying to accomplish
The goal is behavioral change in ordinary life.
Clients need more than insight. They need a repeatable way to get through the moments that have been setting off use, whether that is a fight with a partner, isolation after work, panic symptoms, a payday ritual, or the urge to shut down emotionally. IOP gives people enough clinical contact to identify those patterns and enough real-world exposure to test new responses while support is still active.
In practice, a strong IOP helps clients:
- identify the situations, thoughts, and emotional states that lead to use,
- build coping skills that hold up outside the therapy room,
- create structure during the hours when relapse risk tends to rise,
- address mental health symptoms that can destabilize recovery,
- strengthen family, peer, and community support,
- prepare for the next stage of care instead of ending treatment without a plan.
What it is not
IOP does not replace detox for someone who may be facing serious withdrawal. It also does not work well as a passive program where a person listens, nods, and goes home unchanged.
The trade-off is straightforward. IOP gives more freedom than residential treatment, but that freedom comes with exposure to everyday triggers. For the right person, that is exactly what makes it effective. They can build recovery skills in the same environment where they will need to keep using them. At Paramount Recovery Centers, that process is guided closely so treatment stays personal, clinically grounded, and realistic for life in Massachusetts.
Determining if an IOP is the Right Fit for You
A good IOP fit usually looks like this: you need more than weekly counseling, but you can still live at home, show up consistently, and stay safe between sessions. That decision should be based on current symptoms, relapse risk, medical needs, and what your evenings and weekends look like, not on what sounds less disruptive.

In real clinical work, I look at whether someone can use outpatient treatment as intended. Can they get to sessions, stay grounded enough to participate, and return to a living environment that will not undo the work each night? If the answer is yes, IOP can be a strong level of care. If the answer is no, starting with more structure usually gives the person a better chance.
Formal placement decisions are often guided by ASAM criteria. The goal is simple. Match the person to a level of care that fits withdrawal risk, physical health, mental health stability, readiness for treatment, relapse risk, and recovery environment. People trying to sort through options often benefit from reading how to pick the right PHP or IOP in Massachusetts before they schedule an assessment.
Signs IOP may be a good fit
IOP often works well when several of these are true:
- Withdrawal does not require medical detox: This matters most for alcohol, benzodiazepines, and other substances that can produce dangerous withdrawal.
- Daily life is still intact enough to support treatment: Work, parenting, school, or housing may be strained, but not so unstable that attendance becomes unrealistic.
- Mental health symptoms are serious but manageable in outpatient care: Depression, anxiety, trauma symptoms, or mood swings may be present, but the person can participate safely without hospital-level supervision.
- There is some ability to follow through: Ambivalence is common. Early recovery rarely starts with perfect motivation. What matters is enough willingness to attend, speak truthfully, and practice skills between sessions.
- The home setting is imperfect, not impossible: A person does not need a flawless support system. They do need a place where early recovery has room to take hold.
Dual diagnosis deserves careful attention here. Someone with addiction and panic attacks, trauma, bipolar symptoms, or depression may do very well in IOP if the program treats both conditions together instead of treating substance use as the only issue. At Paramount Recovery Centers, that day-to-day fit matters. Treatment is adjusted around how symptoms show up in real life, including work stress, family conflict, sleep disruption, shame, and the different pressures that often surface in gender-specific groups.
When IOP may not be enough
Some people need a higher level of care first.
That is often true when a person is at risk for severe withdrawal, cannot maintain basic safety, is using in a way that keeps them intoxicated most of the day, has psychiatric symptoms that are acutely unstable, or lives in an environment where access to substances and conflict are constant. In those cases, giving someone too much freedom too early can set them up for a quick relapse and the mistaken belief that treatment did not work.
The problem is often placement, not effort.
A practical self-check
These questions are not a diagnosis, but they help clarify whether IOP is worth assessing right now:
| Self-check question | Why it matters |
|---|---|
| Can you stop using without immediate medical danger? | If not, detox should come first |
| Can you reliably attend several sessions each week? | IOP only helps if you can participate consistently |
| Is your home or sober living setting safe enough for early recovery? | Evening and weekend exposure can either support progress or derail it |
| Are your mental health symptoms stable enough for outpatient treatment? | IOP can treat co-occurring disorders if safety is steady |
| Would gender-specific care or dual-diagnosis support improve your honesty and engagement? | The right clinical setting often makes it easier to talk about trauma, relationships, and relapse patterns |
A professional assessment is still the safest next step. Self-reflection can point you in the right direction, but a qualified team can tell you whether IOP is appropriate now, whether you need a higher level of care first, and what kind of structure will give you the best chance to stay in treatment long enough for it to help.
IOP vs Other Addiction Treatment Levels
People often assume addiction treatment comes in only two forms. Either weekly counseling or full residential rehab. In reality, treatment works on a continuum. IOP sits in the middle of that continuum, and that middle position is exactly why it helps so many adults who need strong support but not constant overnight care.
What matters most is not prestige or intensity for its own sake. What matters is fit.
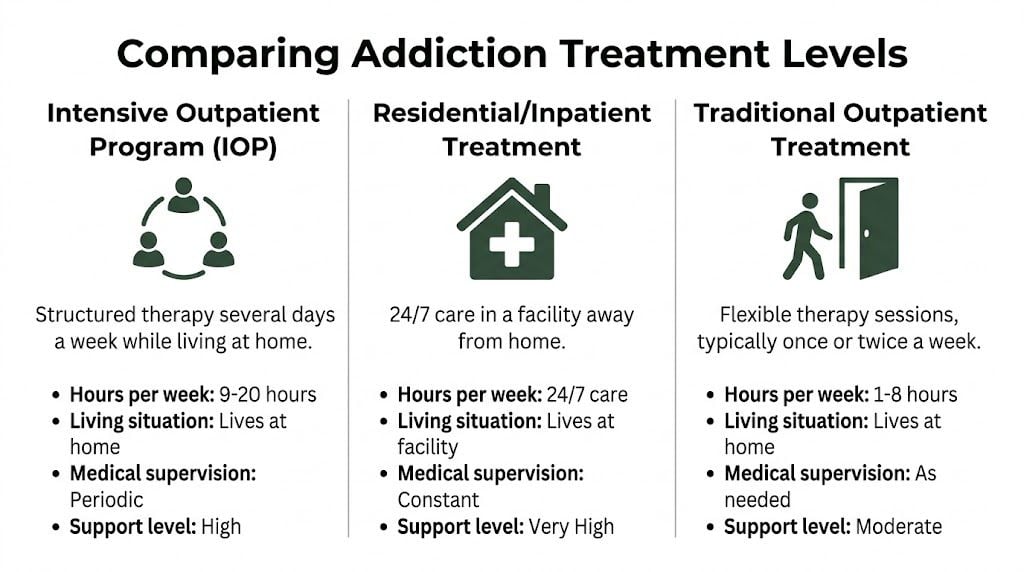
Addiction Treatment Levels of Care Compared
| Level of Care | Time Commitment | Living Arrangement | Best For |
|---|---|---|---|
| Inpatient or Residential | Full-day treatment with overnight stay | Lives at the facility | People who need 24-hour structure, withdrawal management support, or separation from an unsafe environment |
| PHP or Day Treatment | Most of the day, multiple days per week | Lives at home or in supportive housing | People who need more support than IOP but don’t need overnight residential care |
| Intensive Outpatient Program | Several sessions each week | Lives at home or in sober living | People who need substantial treatment while maintaining work, family, or community responsibilities |
| Standard Outpatient | Limited weekly sessions | Lives at home | People who are more stable and need lower-intensity ongoing support |
Where IOP stands clinically
IOP is stronger than many people expect. It’s not a watered-down version of treatment. It’s a legitimate treatment setting with a clear role in the continuum of care.
High-level evidence confirms that IOPs significantly reduce drug and alcohol use, and while some studies show stronger early abstinence rates for inpatient care, those differences often dissipate by the six-month mark, supporting IOP’s comparable long-term efficacy for many individuals in this review of intensive outpatient treatment research.
That matters because people sometimes hear “outpatient” and assume “less effective.” That’s too simplistic. For a person who’s clinically appropriate for IOP, a well-run outpatient program can produce meaningful recovery gains without requiring a residential stay.
The trade-offs are real
Each level of care solves a different problem.
- Residential care offers separation: This can help when a person needs distance from triggers, access to constant supervision, or immediate stabilization.
- PHP provides more daily containment: It’s useful when someone needs more structure than IOP but can still live outside a facility.
- IOP tests recovery in real life: The client attends treatment and then returns to ordinary stressors, relationships, and decisions the same day.
- Standard outpatient preserves flexibility: It works best after stronger stabilization or for people with lower acuity.
That third point is important. IOP’s biggest strength can also be its biggest challenge. People don’t get to practice recovery in a bubble. They leave group and still have to deal with their phone, commute, partner, loneliness, cravings, and old routines. But that real-world exposure is also where skill-building starts to stick.
How to think about the decision
A useful way to choose is to ask what kind of support the person needs between sessions.
If they need someone present overnight, IOP probably isn’t enough. If they only need occasional check-ins, IOP may be more than necessary. If they need a strong therapeutic container while still remaining active in daily life, IOP is often the most practical and clinically sound middle path.
A Glimpse into a Typical Week in an IOP
The unknown keeps many people from enrolling. They hear “intensive outpatient program substance abuse treatment” and imagine something vague, awkward, or impossible to fit into life. The day-to-day experience is usually much more concrete than that.

A typical week has rhythm. Clients know when they’re expected, what kind of sessions they’ll attend, and what they’re working on. That predictability matters because addiction often thrives in chaos, avoidance, and inconsistent routines.
What the week usually includes
A strong IOP schedule often combines several different kinds of treatment rather than repeating the same group every day.
One block may focus on relapse prevention. Another may center on coping skills, thought patterns, or emotional regulation. There’s usually individual therapy built into the week, and family work may be included when clinically appropriate.
The structure seen in evidence-based IOP models reflects that mix. The Matrix approach, for example, emphasizes a strong therapeutic relationship, structured skill-building, relapse prevention groups, social support sessions, family education, and random drug testing within a typical 16-week intensive phase, as outlined in the Matrix model clinical guide.
A sample rhythm
A week might look something like this in practice:
- Early week group session: Clients review triggers from the weekend, discuss current relapse risk, and identify what needs attention before the week gets away from them.
- Skills-focused group: The clinician may use CBT-based work to help clients connect thoughts, feelings, urges, and behavior.
- Individual therapy session: The person can dig into trauma history, family conflict, depression, shame, or resistance that they may not want to unpack in group.
- Psychoeducation block: Clients learn about cravings, withdrawal aftereffects, high-risk people or places, emotional flooding, sleep disruption, or communication habits.
- Recovery planning before the weekend: This often includes a specific plan for downtime, social pressure, transportation, medications, support meetings, and emergency contacts.
What group therapy actually feels like
People often worry that group means forced sharing or public humiliation. In a competent program, it shouldn’t feel like that.
Group is where clients notice they’re not uniquely broken. They hear other people describe the same minimization, secrecy, guilt, rationalizing, and fear that’s been running their own life. That can lower shame fast. It also creates accountability, because peers will often notice avoidance before the client admits it.
Some of the most useful moments in treatment happen when a person hears their own pattern described by someone else.
Why individual therapy still matters
Group can expose patterns. Individual counseling helps organize them.
That’s where a therapist can tailor treatment around co-occurring issues such as trauma, obsessive thinking, panic symptoms, grief, relationship instability, or depressive collapse. For many clients, substance use isn’t the only problem. It’s the coping strategy that developed around untreated pain, chronic stress, or psychiatric symptoms.
The less visible parts of progress
Progress in IOP doesn’t only happen during sessions. It happens at 6 p.m. when a person takes a different route home. It happens when they answer a sponsor, delete a contact, tell the truth to a partner, eat dinner, go to sleep sober, or leave an argument instead of escalating it.
Those changes can look small from the outside. Clinically, they matter a lot. Recovery is usually built through repeated course corrections, not one dramatic breakthrough.
The Paramount Recovery Centers IOP Advantage in Massachusetts
A Massachusetts client leaves work at 5, picks up a child from practice, feels panic rising in the car, and still makes it to evening treatment instead of stopping for a drink or a pill. That is the true test of an IOP. It has to fit real life while helping a person change what happens inside real life.
Paramount Recovery Centers builds its intensive outpatient care around that day-to-day pressure. Clients are not placed into one generic addiction track and expected to adapt on their own. Treatment is shaped around substance use, mental health symptoms, trauma history, family strain, and the practical demands waiting outside the building. For adults with co-occurring disorders, that difference shows up quickly in attendance, honesty, and willingness to stay with the work when treatment gets uncomfortable.
Why dual-diagnosis care changes the day-to-day experience
Anxiety, depression, trauma symptoms, obsessive thinking, mood swings, and sleep disruption can drive substance use and get worse during early recovery. If those symptoms are treated as side issues, people often leave sessions with insight but no workable plan for the hours that trigger them most.
At Paramount Recovery Centers, therapies are chosen based on what is keeping the cycle going. CBT may help a client catch the thought pattern that turns stress into a binge. EMDR can be appropriate when trauma keeps surfacing and the person has enough stability to do that work safely. Family therapy can matter when the home environment is full of secrecy, resentment, or enabling. Medication management support can help when psychiatric symptoms are intense enough to interfere with treatment participation.
That clinical fit affects the patient experience in concrete ways. People stay engaged longer when treatment feels relevant, respectful, and organized around their actual barriers. The broader discussion around improving patient experience applies here too, because trust and clarity influence whether a client tells the truth about cravings, relapse, medication problems, or what happens after sessions end.
Gender-specific treatment can remove barriers that generic groups miss
Some clients speak more openly and do better clinically when treatment addresses gender-specific pressures directly. In practice, I have seen this matter most when shame, trauma, family roles, or identity-based expectations are shaping how a person uses and how they hide it.
For women, treatment may need to account for trauma exposure, caregiving overload, relationship coercion, body image concerns, or mood and sleep disruption tied to hormonal changes in midlife. For men, it may be more important to address emotional suppression, anger, isolation, performance pressure, or the belief that asking for help means weakness. Neither pattern is universal, but both are common enough that good programming should make room for them.
Paramount Recovery Centers offers gender-specific programming for men and women because these themes affect participation. Clients often say they can get to the core issue faster when the room feels clinically relevant to their experience, not just broadly supportive.
What makes the program stronger in practice
The advantage is not one therapy or one schedule. It is the way the pieces work together for the individual client.
- Integrated treatment planning: Substance use and mental health are addressed together, so panic, depression, trauma responses, or compulsive thinking are not treated as separate problems to deal with later.
- Therapy matched to the driver of use: Clients may need skills training, trauma treatment, relapse prevention, family work, or medication support in different proportions at different stages.
- Attention to real-life roles: Care plans can account for parenting, work demands, relationship conflict, transportation issues, and other pressures that often decide whether someone can stay consistent in IOP.
- Aftercare planning before discharge: Recovery support, therapy follow-up, psychiatric care, and relapse planning are built early, not left for the last few days.
For someone considering intensive outpatient treatment in Massachusetts, that is the practical advantage of Paramount Recovery Centers. The program is built to help people function better between sessions, not just inside them.
Measuring Success and Building a Life After IOP
People often ask whether success in treatment only means abstinence. Abstinence matters, but it’s not the only marker worth watching. A person can stop using for a short period and still remain at high risk if nothing else changes around them.
In practice, meaningful success usually looks broader. Sleep improves. Thinking gets clearer. Conflict becomes less explosive. Attendance stabilizes. The person starts telling the truth faster. Cravings become more manageable. Mental health symptoms become easier to track and treat. Daily structure stops feeling impossible.
What clinicians look for
A strong discharge picture often includes progress in several areas at once:
- Substance use stability: fewer return-to-use episodes, better trigger awareness, stronger coping plans
- Mental health improvement: reduced symptom intensity or better management of ongoing symptoms
- Functional recovery: better follow-through with work, school, parenting, appointments, and finances
- Relationship repair: clearer boundaries, more honesty, and less chaos in close relationships
An integrated IOP study involving people with substance use and co-occurring mental health disorders found that 55.6% completed the program, and among completers, satisfaction was very high, with median scores of 10/10 for experience, staff relationships, and personal development in this study on integrated outpatient care. That doesn’t mean every recovery path is smooth. It does show the value of structured, integrated treatment when people stay engaged.
Recovery is often easier to measure by how someone lives than by what they promise.
What happens after the intensive phase
The end of IOP shouldn’t feel like a cliff. It should feel like a step-down.
Aftercare may include ongoing outpatient therapy, medication management, community recovery meetings, alumni support, family work, and a written relapse response plan. Some people also benefit from sober living or continued case coordination while they stabilize employment, housing, or legal issues.
The most important point is simple. Graduation from IOP isn’t the finish line. It’s the point where the person has enough structure, insight, and practice to keep building a life that doesn’t need substances to function.
Frequently Asked Questions about IOP Treatment
How many days a week does IOP usually require
It varies by program and clinical need. In general, IOP involves multiple treatment sessions each week rather than a single appointment. The schedule is meant to provide enough repetition and accountability for real behavior change while still allowing the client to live at home.
Will insurance cover intensive outpatient program substance abuse treatment
Coverage depends on the plan, medical necessity criteria, and network details. Individuals should expect an admissions or verification process before starting. If someone is still sorting out coverage options, practical guidance on how to find affordable health insurance can help them understand the broader insurance environment before they speak with an admissions team.
Can someone work while attending IOP
Often, yes. That’s one of the main reasons people choose this level of care. Many programs offer schedules that can work around employment or family responsibilities, although clients still need enough space in the week to attend consistently and do the work outside sessions.
Does family take part in treatment
Often, yes, when it’s clinically appropriate and the client agrees. Family participation can help repair communication, reduce enabling patterns, and create a more stable recovery environment. It can also help loved ones understand that addiction treatment isn’t just about telling someone to stop. It’s about changing the system around the behavior.
What if the person also has anxiety, depression, trauma, or OCD symptoms
That’s common. Many people entering treatment have co-occurring mental health needs. Those symptoms should be evaluated as part of treatment planning, because recovery is harder to sustain when the emotional and psychiatric drivers behind substance use go untreated.
What is the first step to getting admitted
The first step is a clinical assessment. That conversation helps determine whether IOP is appropriate or whether detox, inpatient treatment, or a higher outpatient level would be safer. It’s also where the treatment team can identify substance use patterns, mental health symptoms, medical concerns, and practical barriers to starting care.
What if someone is unsure they need this much treatment
Uncertainty is normal. People rarely call treatment at their most confident point. They usually call when they know things aren’t working and they’re trying to figure out what level of help fits. That’s exactly what an assessment is for.
If alcohol or drug use is colliding with work, family, or mental health, the next step doesn’t have to be a guess. Paramount Recovery Centers helps adults in Massachusetts figure out whether detox, PHP, or intensive outpatient care is the right fit, with support for dual diagnosis, gender-specific treatment, and ongoing recovery planning. To speak with admissions and explore treatment options, call (888) 388-8660.
