
OCD rarely looks dramatic from the outside. It often looks like a person running late because they had to check the stove again. It looks like someone avoiding a public restroom, a loved one asking for reassurance one more time, or a person lying awake replaying a thought they never wanted in the first place. The suffering is private, repetitive, and exhausting.
That cycle gets even harder when OCD shows up alongside substance use, trauma, or both. Many adults try to calm the anxiety with alcohol, drugs, or rigid routines that offer quick relief but keep the disorder in place. That’s where erp therapy for ocd becomes more than a concept. It becomes a practical way to interrupt the loop and start building a life that isn’t organized around fear.
The Unseen Battle of OCD and How ERP Therapy Can Help
A common pattern looks like this. An intrusive thought lands. Anxiety spikes. The person checks, washes, repeats, confesses, avoids, or asks for reassurance. Relief arrives for a moment, then fades, and the next obsession comes back stronger.
For many people, the hardest part is that they know the ritual doesn’t make sense, but stopping it feels unbearable. That gap between logic and felt danger is where OCD does its best work. A person can understand that a doorknob probably isn’t dangerous and still feel compelled to scrub their hands raw.

Why ERP matters
Exposure and Response Prevention, usually called ERP, is the treatment most clinicians turn to when they want to target OCD directly. Research indicates that approximately 60% to 85% of patients who complete ERP achieve significant success, and it’s recognized as the gold-standard, first-line psychological treatment for OCD by the American Psychiatric Association and the International OCD Foundation, as described in this review of ERP outcomes and clinical guidance.
That matters because people with OCD often spend years trying approaches that reduce stress in the moment but don’t change the disorder itself. General talk therapy may help someone feel understood. Relaxation can lower tension. Insight can be useful. But OCD tends to hold on when treatment doesn’t directly target the obsession-compulsion cycle.
OCD gets stronger when treatment keeps negotiating with fear instead of testing it.
What this means when someone is seeking help
The first useful step is often learning to identify the pattern clearly. A person who isn’t sure whether they’re dealing with OCD can start by reviewing common OCD symptoms and behavior patterns, then seeking a proper clinical assessment.
When OCD is tied to alcohol or drug use, treatment planning needs even more care. Substance use can become a way to blunt anxiety before exposures, escape discomfort after exposures, or avoid treatment entirely. In those cases, the work isn’t just about stopping rituals. It’s about building enough stability that exposure work can take hold.
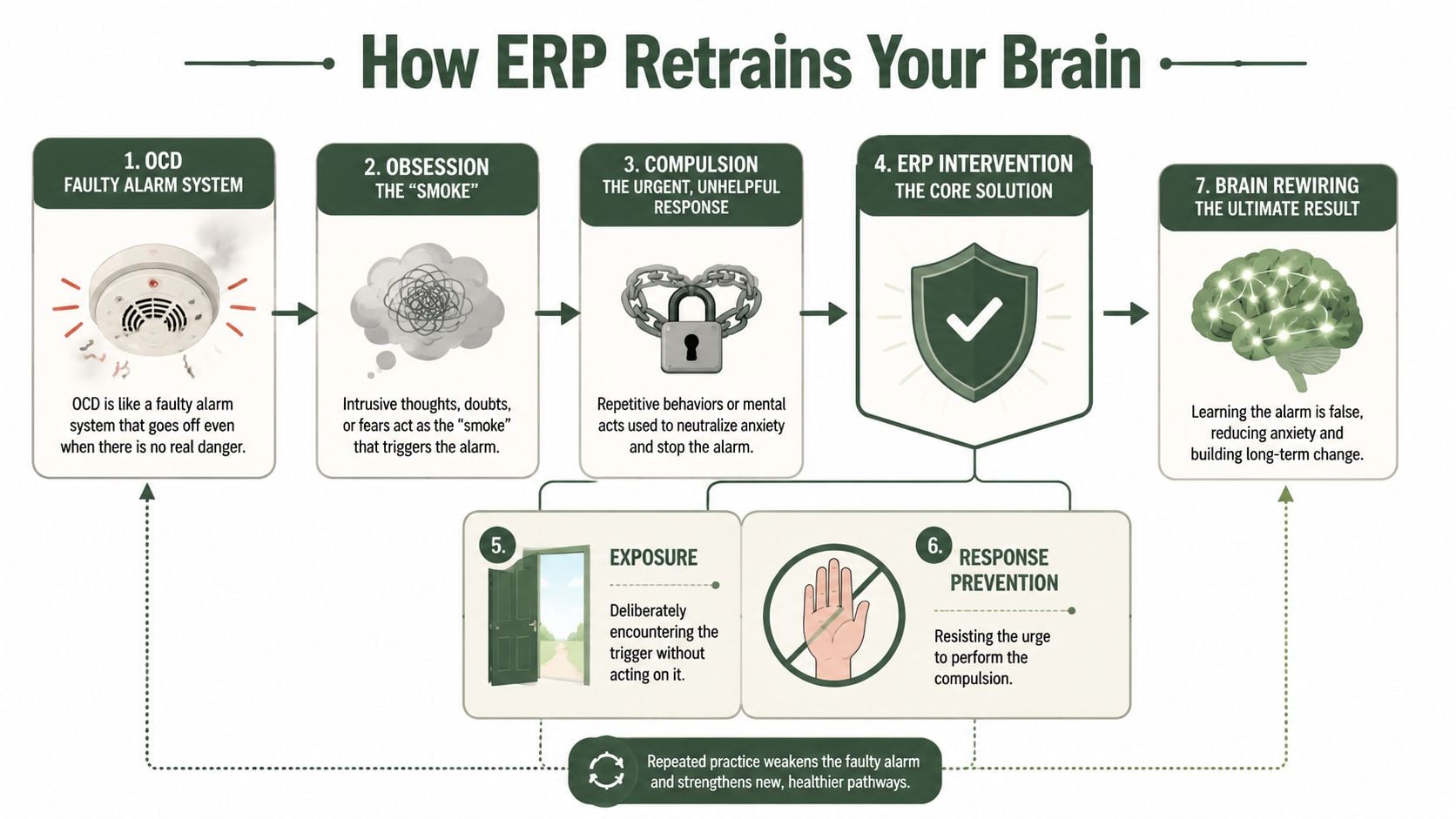
Understanding How ERP Retrains Your Brain
OCD acts like a smoke detector that goes off when there’s burnt toast, steam from the shower, or no smoke at all. The alarm feels urgent, even when there’s no actual fire. The obsession is the alarm signal. The compulsion is the frantic response to shut it off.
ERP doesn’t try to prove the alarm will never sound. It teaches the brain that the signal doesn’t need an emergency response every time it appears.
What actually changes during ERP
ERP works by having a person face a trigger and resist the ritual that usually follows. Over time, that process weakens the learned fear response. According to Palo Alto University’s summary of ERP research and practice, ERP induces habituation of learned anxiety responses and helps extinguish the conditioned fear association by showing the feared consequences don’t occur, which leads to revised threat interpretations. The same source notes that greater insight into OCD symptoms predicts better treatment response, and measurable improvement often occurs within 12 to 20 sessions.
That’s the clinical language. In plain terms, the brain learns, “This thought can show up, and nothing has to be done about it.”
A few examples make that easier to picture:
- Contamination OCD: A person touches a sink handle and doesn’t wash right away.
- Checking OCD: A person locks the door once and leaves without returning.
- Harm obsessions: A person allows an intrusive thought to be present without mentally neutralizing it.
Why the ritual matters more than the feeling
People often assume the goal is to stop anxiety fast. It isn’t. The goal is to stop feeding the rule that says anxiety must be obeyed.
That’s why ERP can feel counterintuitive at first. The treatment asks the client to do less, not more. Less checking. Less certainty-seeking. Less reassurance. Less avoidance. More willingness to let discomfort rise and fall on its own.
Clinical reality: Progress usually starts when the person stops treating uncertainty like a problem that must be solved immediately.
For some clients, related approaches can support the process. Cognitive work may help identify distorted beliefs, and broader OCD and CBT treatment approaches can clarify how thinking patterns and behavior loops interact. But ERP stays focused on the behavior that keeps OCD alive. That precision is why it works when more general coping methods don’t.
The ERP Therapy Process Step by Step
Starting ERP is easier when the process isn’t mysterious. Good treatment is structured. It’s collaborative. It moves with intention rather than forcing a person into feared situations without preparation.
Step 1 involves mapping the OCD system
Early sessions focus on assessment. The clinician identifies the obsessions, compulsions, avoidance patterns, reassurance habits, and situations that trigger distress. The client’s job is honesty, even when the content feels embarrassing or irrational.
This stage often changes how people see their symptoms. Behaviors that seemed unrelated start to fit together. A person may realize that asking a partner for reassurance, rereading texts, avoiding knives, or praying in a rigid way are all part of the same OCD loop.
Step 2 builds a fear hierarchy
ERP usually uses a fear hierarchy, sometimes called a fear ladder. This is a list of triggers ranked from easier to harder. The point isn’t to make treatment comfortable. The point is to make it doable and systematic.
A therapist helps the client choose starting points that are challenging enough to matter but not so overwhelming that the person shuts down. Distress is often rated with a SUDS scale, meaning subjective units of distress.
Here is a simple example:
| SUDS Rating | Exposure Task |
|---|---|
| Low | Touch a kitchen counter and wait before washing |
| Moderate | Touch a public door handle and continue with the day |
| Higher | Handle trash, then delay washing longer than usual |
| Very high | Touch a feared “contaminated” object and eat a snack after standard hygiene only |
Step 3 puts exposures into action
In session, the clinician and client practice exposures together. That might mean touching a trigger, reading a feared statement aloud, intentionally leaving something unchecked, or entering a situation that has been avoided.
The therapist does not rescue the client from anxiety. The therapist coaches the client through it. That distinction matters.
A strong ERP therapist helps with several tasks at once:
- Tracking the ritual urge: noticing when the mind starts bargaining
- Blocking subtle compulsions: catching mental review, silent reassurance, or “just in case” behaviors
- Keeping the exposure clean: making sure the exercise tests the fear instead of watering it down
- Reinforcing willingness: praising the act of staying present, not the absence of anxiety
The measure of success in an exposure isn’t whether anxiety vanished. It’s whether the person stopped performing the old safety ritual.
Step 4 extends the work into daily life
ERP doesn’t work if it only happens in an office. Homework is where learning becomes durable. Clients practice between sessions, track what happened, and review what got in the way.
This part is often where treatment becomes real. Someone with contamination fears may stop using paper towels to open doors at work. Someone with checking rituals may leave the house after one lock check. Someone with taboo intrusive thoughts may stop confessing every mental image to a loved one.
Common homework targets include:
- Reducing reassurance: asking fewer “Are you sure?” questions.
- Dropping avoidance: going places that OCD has narrowed out of life.
- Resisting mental rituals: not replaying, analyzing, or neutralizing thoughts.
- Practicing repetition: doing the same exposure enough times for new learning to stick.
Step 5 shifts toward self-management
As treatment progresses, the client gets better at recognizing OCD quickly and responding with skill instead of panic. Relapse prevention becomes part of the plan. The work isn’t to guarantee that intrusive thoughts never return. The work is to know what to do when they do.
That’s also when clinicians look closely at the wider picture. If trauma reactions, depression, substance cravings, or unstable routines are disrupting ERP, those issues need direct attention rather than being treated like side notes.
What ERP Looks Like in Real Life
Abstract descriptions can make ERP sound sterile. In reality, it’s specific, practical, and adjusted to the kind of OCD a person has.

Contamination fears
A client is afraid that touching public surfaces will lead to illness or spread contamination to family members. Their ritual is handwashing, changing clothes, and wiping down personal items.
The exposure starts small. They touch a waiting room chair and sit with the discomfort. Response prevention is the core treatment. They don’t wash immediately, don’t ask whether the chair looked dirty, and don’t mentally review what they touched.
Over time, the tasks become more ordinary and more meaningful. The goal isn’t reckless behavior. The goal is standard hygiene instead of OCD-driven decontamination routines.
Checking rituals
Another client fears causing harm because of carelessness. Their compulsions include checking locks, appliances, and messages repeatedly. They know the lock is engaged, but the doubt won’t release them.
An ERP exercise might involve locking the door once, saying “maybe it’s locked, maybe it isn’t,” and walking away. That phrase matters because it interrupts the hunt for certainty. The response prevention includes no returning, no calling someone to verify, and no replaying the image of the lock in their head.
Intrusive harm or taboo thoughts
This form of OCD is often hidden because the content feels shameful. The person may fear they are dangerous, immoral, or secretly want what they fear. Their compulsions are usually mental. They analyze thoughts, pray in a rigid way, confess, avoid people, or seek reassurance that they aren’t “that kind of person.”
In those cases, ERP may use imaginal exposure. The client writes and reads a script that describes the feared uncertainty, then listens to it without neutralizing. The point isn’t to agree with the fear. The point is to stop performing rituals to prove the fear false.
Many people with taboo or harm obsessions don’t need more reassurance that they’re safe. They need treatment that stops the compulsive need to prove it.
What these examples have in common
The content changes, but the structure stays steady:
- A trigger is chosen on purpose
- The ritual is identified clearly
- The person stays in contact with uncertainty
- Learning happens because the old escape route is blocked
That’s why ERP can be adapted across OCD subtypes without becoming generic. It stays grounded in what the person does when fear appears.
Integrating ERP with Other Treatments and Needs
ERP is powerful, but it isn’t magic and it isn’t always enough by itself. Some clients improve when ERP directly targets rituals and avoidance. Others need a broader plan because trauma, shame, overcontrol, mood symptoms, or substance use keep interfering with the exposure process.
Research summarized in this review of integrated treatment considerations for OCD notes that 60 to 70 percent of patients respond well to ERP, while integrated treatment is important for the rest. That same summary explains that supplementing ERP with cognitive work, emotion regulation skills, and treatment that addresses trauma and shame can produce better outcomes than ERP alone. It also notes that certain medications may accelerate ERP progress, though that requires careful management in clients with co-occurring substance use disorders.
Why dual diagnosis changes the treatment plan
A person with OCD and substance use may use alcohol to lower anxiety before exposures, sedatives to sleep after distress, or stimulants to outrun intrusive thoughts. That can make treatment look inconsistent when the actual issue is that the nervous system and reward system are being pulled in different directions.
Trauma can complicate things in a different way. Some clients don’t only fear uncertainty. They also react to exposure with intense shame, dissociation, or a survival-state response that needs separate clinical attention. If a therapist treats every spike in distress as simple OCD anxiety, treatment can miss the mark.
Practical adjustments may include:
- Sequencing care carefully: addressing withdrawal, stabilization, or unsafe substance patterns before intensive exposure work
- Using emotion regulation skills: helping the client stay present without turning exposures into overwhelm
- Adding cognitive interventions: targeting beliefs about responsibility, danger, guilt, or the meaning of thoughts
- Including family work: reducing reassurance cycles and accommodation at home
What doesn’t work well
ERP loses strength when it becomes too diluted. Common problems include turning exposures into discussions, allowing hidden rituals to continue, or moving so fast that the client spends the week recovering rather than practicing.
It also tends to stall when treatment ignores the person’s full context. A client in early sobriety may need pacing, medical oversight, and close coordination. A client with trauma may need a plan that distinguishes an OCD trigger from a trauma trigger. A client drowning in shame may need direct work on self-judgment so they can participate openly.
One treatment option that addresses these overlapping needs is care focused on treating OCD without medication when clinically appropriate, alongside dual-diagnosis programming, behavioral therapy, and coordinated support when medication is part of the plan.
Your Questions About ERP Therapy Answered
Is ERP too scary for most people
ERP is challenging, but good ERP isn’t reckless. The therapist doesn’t start with the hardest fear and “flood” the client. The work is graded, planned, and collaborative. The point is to build willingness and consistency, not to shock someone into change.
How long does it take to notice progress
Many people want a precise timeline. The honest answer is that it depends on symptom pattern, severity, motivation, hidden rituals, and whether other conditions are interfering. Some people notice meaningful shifts early when they engage fully. Others need more time because the rituals are subtle or because trauma and substance use complicate the work.
Can someone do ERP alone
Self-help can increase awareness, but OCD is skilled at disguising compulsions as coping. People often think they’re doing exposure while reassuring themselves, modifying the task, or avoiding the core fear. That’s why trained guidance matters. A clinician can spot the ritual the client doesn’t realize they’re still doing.
A home practice plan can support ERP. It usually shouldn’t replace professional assessment and coaching.
Does ERP work for thoughts, not just visible rituals
Yes. Many compulsions are mental. Reviewing, praying in a rigid way, confessing, seeking certainty, or trying to “cancel out” a thought can all become treatment targets. ERP can be adapted for those patterns through imaginal work and response prevention aimed at mental rituals.
What if OCD is mixed with addiction or trauma
That calls for a more careful treatment model, not less hope. The key question is whether the care team can separate OCD from withdrawal, panic, trauma reactions, and craving patterns while still keeping ERP active. When treatment can do that well, clients are far more likely to stay engaged.
Start Your Recovery with Expert ERP at Paramount Recovery Centers
OCD is treatable. It’s treatable in a way that directly targets the cycle that keeps life small. ERP asks a person to stop obeying fear, one step at a time, until the rituals lose their authority.
That process becomes more complex when OCD is tangled with alcohol use, drug use, trauma, shame, or unstable mental health symptoms. In those cases, generic care often misses the interaction between the disorders. A client may need exposure work, substance use treatment, family support, medication coordination, and skills for regulating distress, all moving in the same direction.
Paramount Recovery Centers provides Massachusetts adults with dual-diagnosis care that can include ERP within a broader treatment plan, along with structured outpatient support, trauma-informed therapy, and coordination around recovery needs that complicate OCD treatment. For a person whose rituals, intrusive thoughts, or avoidance have taken over daily life, the next useful step is a clinical conversation that looks at the full picture rather than one symptom in isolation.
For help evaluating treatment options, insurance, and level of care, call (888) 388-8660.
Paramount Recovery Centers helps adults in Massachusetts access care for OCD, addiction, trauma, and other co-occurring mental health concerns through a full continuum of treatment. To speak with an admissions specialist, verify insurance, or discuss whether ERP may fit a broader recovery plan, contact Paramount Recovery Centers at (888) 388-8660.
