
OCD can take over a day before the day has even started. A person wakes up and already feels behind, not because of work or family demands, but because the mind has started bargaining. Check the stove one more time. Replay that conversation again. Wash again. Pray again. Ask for reassurance again. By noon, hours are gone and shame has usually joined the anxiety.
Many adults who reach out for help in Massachusetts say the same thing in different words. They are exhausted, scared of what their thoughts might mean, and unsure whether medication is the only option. Some want to avoid medication entirely. Others have tried it before and did not get the life change they hoped for. What they need is a clear answer to a practical question: how to treat OCD without medication in a way that is structured, evidence-based, and realistic.
That path exists. It is not passive, and it is not quick self-help dressed up as treatment. It usually involves targeted psychotherapy, repeated practice, family or social support, and a long-term plan for maintaining gains. Done well, non-medication treatment can help people interrupt the obsession-compulsion cycle, tolerate uncertainty, and return to ordinary decisions without hours of rituals or avoidance.
Reclaiming Your Life from Obsessive-Compulsive Disorder
A person with contamination OCD may know, intellectually, that a clean countertop is probably safe. Yet the body still reacts as if danger is present. Another person with harm obsessions may love their family and still feel trapped by violent intrusive images they never wanted. Someone with checking OCD may leave the house, turn around, and lose another half hour to a lock, a stove, or a text message that “needs” one more review.
That is why OCD feels so confusing. It does not create fear. It hijacks attention, time, and trust in one’s own judgment.

The good news is that people do recover without relying on medication alone, and many recover without medication at all. The turning point is usually not finding the perfect reassuring thought. It is learning a different response to obsessional doubt. Instead of obeying the urge to neutralize fear, the person practices staying present, resisting rituals, and letting anxiety rise and fall without solving it.
Key takeaway: Non-medication OCD treatment works when it changes behavior, not when it chases certainty.
This is difficult work, but it is teachable work. The process often starts with understanding what helps, what tends to backfire, and when specialized care is necessary. For adults dealing with OCD alongside trauma, alcohol use, drug use, or severe functional impairment, that level of care matters even more. A strong plan does not just reduce symptoms. It gives a person their day back.
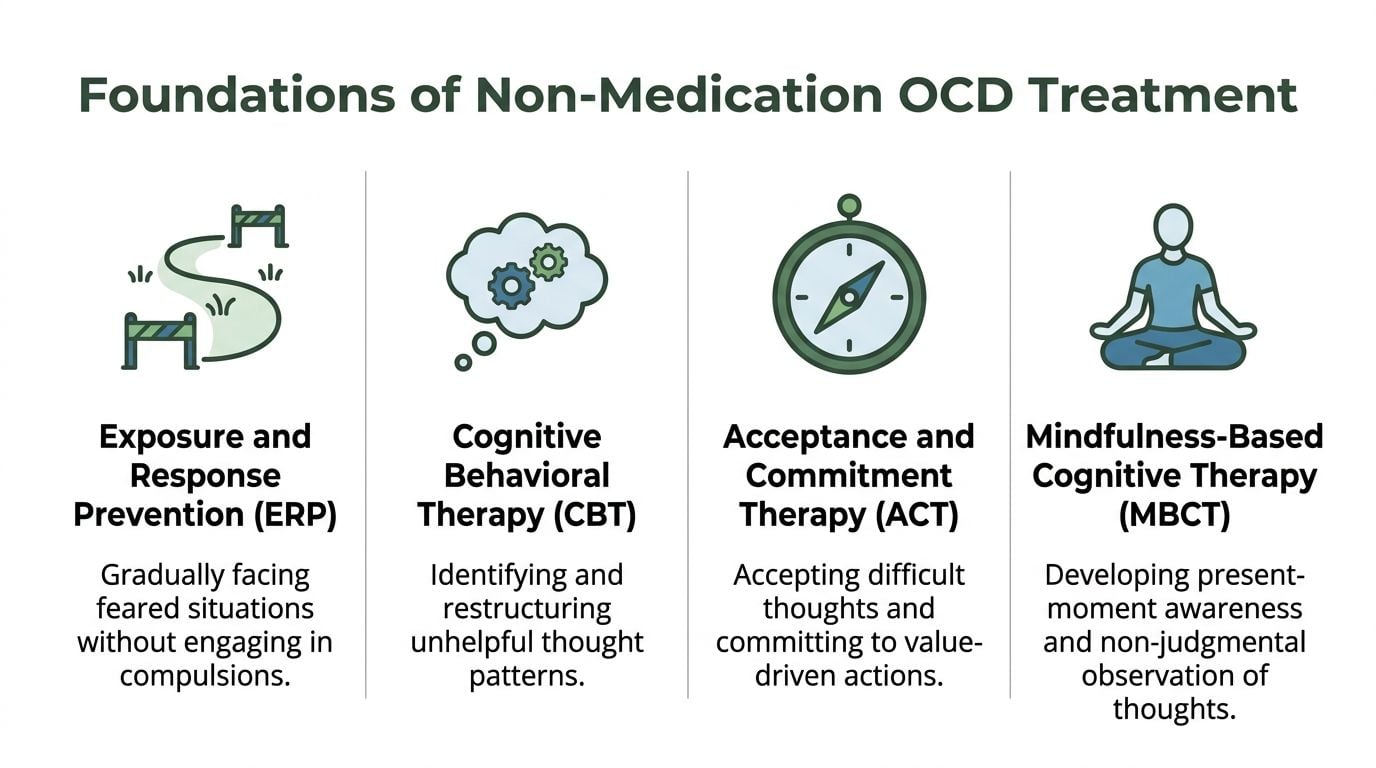
The Foundations of Non-Medication OCD Treatment
A good non-medication OCD plan starts with one hard truth. Feeling better in the moment is not the same as getting better.
Many people come into treatment after months or years of doing what seems reasonable. They avoid triggers. They ask for reassurance. They review, confess, check, pray, wash, or mentally argue with a thought until the panic drops. The short-term relief is real. The long-term cost is also real, because each ritual trains OCD to come back louder the next time.
The treatment that most often changes that pattern is Exposure and Response Prevention, or ERP. ERP is the central behavioral treatment for OCD, and it works by helping a person face triggers without performing the ritual that usually follows. For many patients, that becomes the backbone of a plan built without medication.
ERP is not generic anxiety advice. It is structured, specific, and personalized.
How ERP changes the cycle
In practice, ERP means identifying a trigger, entering that situation on purpose, and then blocking the compulsion. The person stays with the discomfort long enough to learn something new. Anxiety rises, shifts, and eventually comes down without the ritual. Just as important, the person learns that uncertainty can be carried without handing control to OCD.
Here is what that looks like in real life:
- Contamination OCD: touching a doorknob, then waiting instead of washing immediately.
- Checking OCD: locking the door once and leaving without returning to confirm.
- Scrupulosity: allowing doubt about whether a prayer or moral action was done “right enough.”
- Relationship OCD: noticing the urge to analyze feelings and choosing not to run the analysis.
What works for OCD often feels counterintuitive at first.
Patients often tell me ERP feels wrong before it feels useful. That reaction makes sense. OCD has usually spent years teaching them that rituals prevent harm, guilt, or catastrophe. ERP asks them to test that rule directly, in a planned way, with support and repetition. The trade-off is uncomfortable at the start, but it gives people something reassurance never does. Actual freedom.
What CBT adds to treatment
CBT helps identify the beliefs that keep OCD stuck. Common themes include inflated responsibility, intolerance of uncertainty, perfectionism, and treating intrusive thoughts as meaningful evidence.
That matters, but CBT for OCD has to stay tied to behavior. A patient may understand, at an intellectual level, that the fear is exaggerated and still feel compelled to ritualize. Insight helps. Repeated practice changes the pattern.
For readers trying to understand how these approaches fit together, this overview of OCD and CBT treatment explains how cognitive work can support exposure-based treatment without replacing it.
Where ACT fits
Acceptance and Commitment Therapy, or ACT, helps when a person gets stuck trying to control thoughts before living their life. The focus shifts from eliminating distress to making room for distress while choosing actions that match the person’s values.
That shift is useful in OCD because the disorder keeps asking for certainty that no one can produce. A parent with intrusive harm thoughts may want proof that they would never act on the thought. A person with religious obsessions may want proof that they have not offended God. ACT helps them stop organizing their day around getting that proof.
The goal is not to like the thought or agree with it. The goal is to notice it, allow the discomfort, and continue with the next right action.
Building a treatment plan from the ground up
The strongest non-medication plans are individualized. They usually include one primary therapy, daily practice between sessions, and a clear decision about what level of care is needed.
A practical plan often includes:
| Treatment element | What it does | How it is used in a personalized plan |
|---|---|---|
| ERP | Reduces compulsions and avoidance through direct practice | Forms the core treatment target list and exposure hierarchy |
| CBT strategies | Identifies distorted beliefs that fuel rituals | Helps sharpen exposures and reduce mental rituals disguised as “problem-solving” |
| ACT skills | Increases willingness to feel uncertainty and distress | Helps patients continue exposures without waiting to feel ready |
| Family or partner guidance | Reduces reassurance and accommodation at home | Prevents loved ones from accidentally strengthening OCD |
| Routine tracking | Shows where rituals are still hiding in daily life | Helps adjust the plan based on patterns at work, home, school, or church |
This is also where specialized care matters, especially for adults with severe avoidance, heavy family accommodation, co-occurring substance use, trauma symptoms, depression, or major disruption at work or school. General mental health support can help a person feel understood. OCD treatment requires a narrower skill set. A free anxiety education hub can help readers understand anxiety patterns, but OCD usually improves fastest when the plan is built and supervised by a clinician who treats OCD directly.
A solid foundation is simple to describe and harder to do. Choose treatment methods that interrupt rituals, build a plan around your actual triggers, and get specialized help early if OCD is running your schedule, relationships, or ability to function.
Mastering Daily Techniques for Managing OCD
A person with OCD can know exactly what the disorder is doing and still lose 45 minutes at the sink, the door, or inside a loop of mental review. Daily management starts there. In the ordinary moment when OCD demands certainty, relief, or reassurance.
The work in this phase is practical. Build daily exercises that fit real triggers, run them in a repeatable way, and catch the hidden rituals that keep symptoms alive between therapy sessions.
Build a fear hierarchy you can use
A fear hierarchy is a working list of triggers ranked from manageable to harder. It should be specific enough that you can practice it today, not someday.
For contamination OCD, a usable hierarchy might include:
- Touch the kitchen counter and wait ten minutes before washing.
- Touch the doorknob at home and eat a snack without rewashing.
- Touch a public door handle and continue the next task without sanitizing.
- Use a public restroom and leave after a standard hand wash, not a ritualized one.
For checking OCD, the list may include locking the door once and walking away, sending an email without repeated rereading, or driving home without circling back to make sure no accident occurred.
Good hierarchies are concrete. “Reduce anxiety” is too vague to practice. “Touch the mailbox and do not wash until after dinner” gives the brain a chance to learn something new.
I usually advise patients to choose one exposure they can complete consistently for several days before moving up. Starting too high often turns treatment into a test of endurance instead of a learning exercise.
Run exposures in a way that changes the pattern
Exposure and Response Prevention works when the exposure is clear and the response prevention is complete. The sequence matters.
- Choose one trigger on purpose. Pick a task from the hierarchy that feels difficult but doable.
- Name the rule before you begin. Decide what you will not do afterward. No checking, no reassurance text, no mental review, no “just this once” ritual.
- Enter the trigger fully. Touch the object, leave the house, send the email, sit with the intrusive thought, or continue driving.
- Stay in contact with the discomfort. Let the anxiety rise and fall on its own while you remain in the situation or continue the task.
- Block every version of the compulsion. This includes silent rituals such as reviewing, counting, praying for certainty, or asking yourself if the exposure “worked.”
- Record what happened. Note the trigger, the urge, what ritual OCD demanded, and what you did instead.
That process sounds simple on paper. In real life, people get stuck in partial response prevention.
Common examples include:
- Stopping the visible ritual but keeping the mental one: No hand washing, but twenty minutes of reviewing whether contamination occurred.
- Doing the exposure, then asking for reassurance: Touching the feared object, then texting a partner for confirmation that everything is fine.
- Turning the exercise into a safety routine: Repeating the same exposure only when conditions feel controlled.
- Leaving before the learning happens: Escaping as soon as distress spikes.
A useful rule in clinic is straightforward. If OCD still gets a ritual at the end, the brain has not learned the lesson you wanted it to learn.
For readers who want a clearer sense of how clinicians structure exposures and homework, this guide to ERP for OCD treatment explains the process in a practical way.
For readers looking at how repeated daily practice shapes behavior over time, this short piece on Mastering Habit Formation Psychology can be a useful companion to exposure work.

Use a brief script when OCD surges
In the moment, people need language they can use quickly. A short script helps create distance from the urge without arguing with it for half an hour.
A practical version looks like this:
Relabel
Call the experience what it is.
“This is an OCD obsession.”
“This is a compulsion urge.”
“This feeling is intense, but it is not evidence.”
Reattribute
Place the urgency where it belongs. In the disorder, not in the situation.
A person with harm OCD may feel driven to analyze whether a thought means danger. A better response is to recognize the false alarm and stop treating the thought like a confession or prediction.
Refocus
Return to the next real task for a set period of time.
Answer the email. Finish loading the dishwasher. Keep walking into the store. Continue the drive. The goal is not to erase anxiety. The goal is to stop serving OCD.
Revalue
After the wave passes, reduce the importance you assign to the obsession.
It was noise.
It was an urge.
It did not deserve a ritual.
This kind of script works best when it supports exposure practice, not when it becomes another mental ceremony. If a person repeats the words for relief until they feel “just right,” OCD has changed clothes.
Use grounding to stay present, not to neutralize fear
Grounding can help during daily practice. It should keep attention anchored in the present while you resist compulsions. It should not become a hidden method for forcing anxiety down.
Useful options include:
- Sensory grounding: Identify five things you see, four you feel, and three you hear while staying in the situation.
- Steady breathing: Slow the pace of breathing without checking whether anxiety is disappearing.
- Object focus: Hold a bead, coin, or textured object while continuing the exposure.
- Body awareness: Notice tension in the jaw, chest, or hands without trying to fix it immediately.
The test is simple. If the skill helps you remain in the exposure and continue normal behavior, keep it. If the skill becomes a private ritual you must complete before you can function, it needs to be revised.
Daily techniques work best when they are written down, practiced on schedule, and reviewed. Patients who improve usually do not wait to feel confident first. They practice with uncertainty, catch the small rituals, and repeat the plan often enough that OCD loses control of ordinary life.
Building Your Personalized Long-Term Recovery Plan
A long-term OCD plan has to work on a Tuesday morning, not just in a therapy session. This is tested when you are late for work, your child is sick, you are traveling, or a familiar trigger shows up after a hard week. If the plan only works under ideal conditions, OCD will find the gaps.
I tell patients to build recovery the way they would build any stable routine. Start with what you can repeat, measure, and adjust. A personalized non-medication plan should fit the actual shape of your life in Massachusetts, including commute demands, family roles, school schedules, weather disruptions, and access to specialized care.
Build around your pattern, not someone else’s
Two people can both have OCD and need very different recovery plans. One person may lose hours to checking before leaving home. Another may function well at work but spend the evening trapped in mental review, reassurance-seeking, or confession rituals. A useful plan names the exact places where OCD takes time, steals attention, and pulls other people into the cycle.
Start by mapping four areas:
- Your main triggers: contamination, harm, scrupulosity, relationship doubt, health fear, perfectionism, or a mixed pattern
- Your usual compulsions: visible rituals, avoidance, reassurance, online searching, confessing, rumination, or silent mental review
- Your high-risk times: waking up, bedtime, transitions, conflict, illness, being alone, deadlines, or travel
- Your support system: who helps recovery, who accidentally accommodates symptoms, and who should know the plan
That map becomes the foundation for treatment choices, daily practice, and relapse planning.
Keep the weekly plan simple enough to follow
Patients often stall because they write a plan that looks disciplined on paper and collapses by day three. A better plan is specific, limited, and realistic.
For many people, a workable week includes:
- One primary exposure goal: a single target to practice repeatedly until it loses some of its power
- One response prevention rule: a clear limit such as no checking locks again, no asking a partner for reassurance, or no replaying the event in your head
- One scheduled review period: a brief written check-in to track wins, missed compulsions, and trouble spots
- One support step: a therapist appointment, family check-in, peer support, or aftercare contact
That structure sounds basic because basic works. Repetition changes the pattern.
Add daily supports that make ERP easier to sustain
Lifestyle structure does not treat OCD on its own. It does affect how well a person can stay with exposure work and resist rituals during stress.
The supports that help most are ordinary:
- Regular sleep: poor sleep makes intrusive thoughts feel louder and harder to dismiss
- Consistent meals: hunger can increase irritability and reduce frustration tolerance
- Physical activity: movement can lower overall stress and improve follow-through with planned exposures
- Predictable routines: fewer avoidable disruptions means fewer openings for compulsive drift
I have seen patients make real gains once they stopped chasing a perfect wellness routine and committed to a stable one. Seven good nights of sleep and three planned walks each week will usually help more than a burst of motivation followed by chaos.
Write a relapse plan before you need one
Relapse prevention should be built into the first version of the plan. OCD commonly returns through small permissions. Extra checking. A little more avoidance. One reassurance question that turns into ten.
A strong relapse plan answers three practical questions:
What shows me OCD is gaining ground?
Look for longer routines, more mental review, rising avoidance, irritability when reassurance is not available, or the return of “just in case” behavior.What do I do in the first 48 hours?
Restart one lower-level exposure, tighten the response prevention rule, reduce family accommodation, and return to written tracking.Who gets notified?
Your therapist, partner, family member, sponsor, or trusted support person should know what early backsliding looks like for you.
Long-term recovery principle: The goal is to respond to spikes early, before they become a full return to compulsive living.
Include family and environment in the plan
OCD often recruits the household. A partner answers reassurance questions. A parent participates in checking. A roommate changes routines to lower your anxiety. These responses usually come from care, but they can keep the disorder in place.
A long-term plan should spell out what support looks like. For example, a spouse may agree to encourage exposure practice but stop answering certainty-seeking questions. A parent may help with transportation to therapy while refusing to participate in rituals. Clear roles reduce conflict and make progress easier to maintain.
Know when self-management is no longer enough
Some people can start this work on their own and make steady progress. Others need specialized help early, especially if OCD is severe, time-consuming, mixed with depression or substance use, or built around hidden mental compulsions that are hard to track without outside guidance.
If you live in Massachusetts, part of a personalized plan should include knowing where you would turn if symptoms intensify. Do not wait for a full collapse in functioning. The better move is to seek specialized OCD care when your home plan stops working, your world starts shrinking, or the people around you are getting pulled deeper into the rituals.
Long-term recovery is built, reviewed, and revised. That is how non-medication treatment becomes durable.
How Professional Guidance Transforms Your Recovery Journey
Self-help can open the door. It rarely replaces specialized care when OCD is severe, complicated, or tangled up with substance use, trauma, depression, or panic. The reason is simple. OCD is skilled at disguising compulsions as safety, morality, responsibility, insight, or even treatment itself.
A person may think they are doing exposure when they are flooding themselves and then escaping. Another may believe they are refusing rituals while continuing covert mental compulsions all day. Someone with substance use may use alcohol or drugs to get through obsessional distress, which can temporarily blunt symptoms while worsening functioning and reinforcing avoidance.
That is where professional guidance changes the outcome.

What a trained clinician does that self-help cannot
A skilled OCD clinician does more than explain ERP. The clinician identifies the rituals the person cannot see clearly, calibrates exposures so they are challenging but doable, and blocks treatment-interfering behaviors that masquerade as coping.
That includes several tasks:
- Case formulation: Sorting obsessions, compulsions, avoidance, reassurance, and accommodation into a treatment map.
- Hierarchy design: Choosing exposures that build learning instead of panic and dropout.
- Response prevention coaching: Catching subtle rituals, especially mental compulsions.
- Accountability: Following up when OCD bargains, stalls, or shifts themes.
- Risk differentiation: Distinguishing OCD content from actual intent, psychosis, trauma responses, or substance-related issues.
This matters even more in dual-diagnosis treatment. If a person uses alcohol, cannabis, sedatives, or stimulants to escape OCD distress, those patterns must be treated alongside OCD rather than as separate problems.
Why integrated care matters in Massachusetts
Adults seeking help in Massachusetts often need more than outpatient talk therapy. Some are trying to manage OCD while also dealing with alcohol misuse, prescription misuse, relapse risk, trauma symptoms, or unstable daily functioning. In those cases, a higher level of support can make the difference between temporary insight and real behavior change.
One option in Massachusetts is Paramount Recovery Centers, which provides dual-diagnosis treatment across levels of care and integrates therapies such as ERP, CBT, EMDR, relapse prevention, family work, and aftercare for adults with co-occurring mental health and substance use concerns.
That kind of structure helps when symptoms do not stay neatly inside one diagnosis. A person with contamination OCD and alcohol use needs a plan for both compulsions and drinking triggers. A person with trauma and intrusive thoughts may need exposure work paced in a way that is trauma-informed rather than blunt or generic. A person who cannot stop seeking reassurance from a partner may need family involvement so home stops feeding OCD.
When non-medication does not mean doing it alone
Some readers searching how to treat ocd without medication assume the choice is between pills and complete self-reliance. That is a false choice. Many people do best with non-medication treatment plus high-quality professional support.
Professional support also helps families stop accidentally strengthening symptoms. Loved ones often participate in rituals because they want to reduce suffering. They answer the same question again, clean “one more time,” avoid ordinary situations, or give moral reassurance. Without guidance, compassion can become accommodation.
A clinician helps the household shift from soothing OCD to supporting recovery.
Advanced options for treatment-resistant OCD
Some people do substantial ERP work and still remain highly impaired. For 40 to 60 percent of OCD cases that do not respond to first-line therapies, Transcranial Magnetic Stimulation (TMS) offers a medication-free option. It was approved by the FDA for OCD in 2018, and response rates in treatment-resistant patients are 30 to 50 percent (iocdf.org/ocd-treatment-guide/).
TMS is not a substitute for a careful diagnostic assessment. It is also not the first move for many. But for the right patient, it can fill an important gap in care, especially when standard therapies have been done well and progress remains limited.
When medication may still be part of the conversation
The question is not whether medication is good or bad. The question is what the individual needs. Some people want a non-medication plan and do well with it. Others begin there and later decide to add medication. Others need enough symptom relief to participate in ERP effectively.
A careful clinician should be able to hold all three truths:
- Medication is not the only path.
- Medication is not a failure.
- Therapy remains central if the goal is lasting behavioral change.
The strongest treatment relationships do not force a single ideology. They build a plan that fits symptom severity, co-occurring conditions, risk, motivation, and access to support.
When to seek specialized help now: daily rituals are consuming hours, work or relationships are suffering, intrusive thoughts feel unbearable, substances are being used to cope, or previous therapy has not targeted OCD directly.
For adults in Massachusetts, the next step should be simple. Reach out, get assessed, and find out whether a structured non-medication OCD plan fits the current level of need. Confidential support is available through admissions at (888) 388-8660.
Frequently Asked Questions About OCD Treatment
How long does ERP take to start working
ERP is not instant, but it is often effective when done consistently and correctly. The verified data on ERP describes treatment as typically unfolding over 12 to 20 weekly sessions in standard psychotherapy delivery, though actual timelines vary by severity and complexity (pmc.ncbi.nlm.nih.gov/articles/PMC9978117/). People usually notice progress when they are completing exposures regularly and stopping rituals, not when they are only reading about treatment.
Can OCD be cured completely
“Cure” is not the most useful frame. The better question is whether symptoms can become manageable enough that they no longer run the person’s life. For many people, the answer is yes. The goal is durable remission, strong self-management, and the ability to respond quickly if symptoms return.
Can family help, or do they make it worse
Both can happen. Family support is powerful when loved ones learn how to stop accommodating rituals and start reinforcing treatment goals. Family involvement can also backfire when relatives provide repeated reassurance, participate in checking, or help a person avoid triggers. A structured treatment plan shows family members what support should look like.
What if intrusive thoughts feel too disturbing to talk about
That is common in OCD. Many people fear disclosure because they mistake intrusive content for intent or character. A trained OCD clinician understands that unwanted thoughts can be ego-dystonic and terrifying without reflecting what a person wants. This overview on intrusive thoughts can help readers understand that difference before treatment begins.
What makes treatment different when OCD overlaps with substance use or trauma
The treatment plan has to address all active drivers at the same time. A person cannot make steady progress with compulsions if substances are being used to escape every spike in anxiety. Trauma also changes pacing, trust, and the need for careful assessment. Integrated care is usually more effective than trying to split these problems apart.
Is non-medication treatment strong enough
Yes, when it is specialized and done well. Properly implemented ERP by a skilled therapist produces significant improvement in about 80 percent of patients, defined as at least a 35 percent reduction on Y-BOCS (psychologytoday.com/us/blog/think-well/201406/how-beat-ocd-without-drugs-its-simple-not-easy). The critical issue is quality and consistency, not just effort.
If OCD is dictating routines, relationships, or the way each day begins and ends, the next step is a clinical assessment, not more silent suffering. Paramount Recovery Centers helps adults in Massachusetts address OCD alongside trauma, substance use, and other co-occurring concerns through evidence-based, individualized care. To speak with an admissions specialist confidentially, call (888) 388-8660.
