

Typing “emdr therapy near me” usually happens at a hard moment. Someone may be tired of feeling hijacked by a memory, stuck in panic, numb after years of carrying too much, or relying on alcohol or drugs to get through feelings that never seem to settle. The search itself is often a sign that talk alone hasn't fully helped, or that the problem finally feels too costly to keep managing alone.
EMDR can be a strong next step. It isn't vague, and it isn't about being forced to relive everything in detail. It's a structured therapy designed to help the brain process experiences that seem frozen in place. For many people in Massachusetts, especially those dealing with both trauma and substance use, that matters because the trauma often keeps feeding the addiction even when the person wants to stop.
Your Search for EMDR Therapy Acknowledged
Searching for emdr therapy near me means a person is already doing something important. They're trying to move from surviving to treating the actual source of distress. That deserves respect.
EMDR stands for Eye Movement Desensitization and Reprocessing. It was developed by Dr. Francine Shapiro in 1987, later became a structured eight-phase psychotherapy protocol, and by 1995 it had been designated by the American Psychological Association as an “effective treatment for PTSD” after a task force review. A landmark 2013 meta-analysis of 26 randomized controlled trials found EMDR significantly more effective than no-treatment and comparable to or exceeding CBT for PTSD symptom reduction, and the World Health Organization endorsed it as a first-line therapy for PTSD in 2013, as described in this overview of EMDR's development and recognition.
For someone looking locally in Massachusetts, the question usually isn't just “What is EMDR?” It's “Can this help with what keeps happening to me?” In many cases, yes. EMDR is often used when a person feels intense reactions that don't match the present moment because the nervous system is still reacting to the past.
What people are often looking for
- Relief from triggers: A smell, argument, anniversary, or relationship dynamic may bring back a level of distress that feels immediate and overwhelming.
- A treatment that isn't endless retelling: Many people want trauma therapy without having to explain every detail over and over.
- Help that fits real life: If trauma and addiction are intertwined, treatment needs to address both, not just one.
A good trauma treatment should help a person feel more present in daily life, not more trapped in old material.
Some readers also want a plain-language explanation before reaching out. This short article on expert trauma therapy can be helpful for understanding what high-quality trauma-informed care should feel like from the client side.
What Is EMDR and How Does It Reprocess Trauma
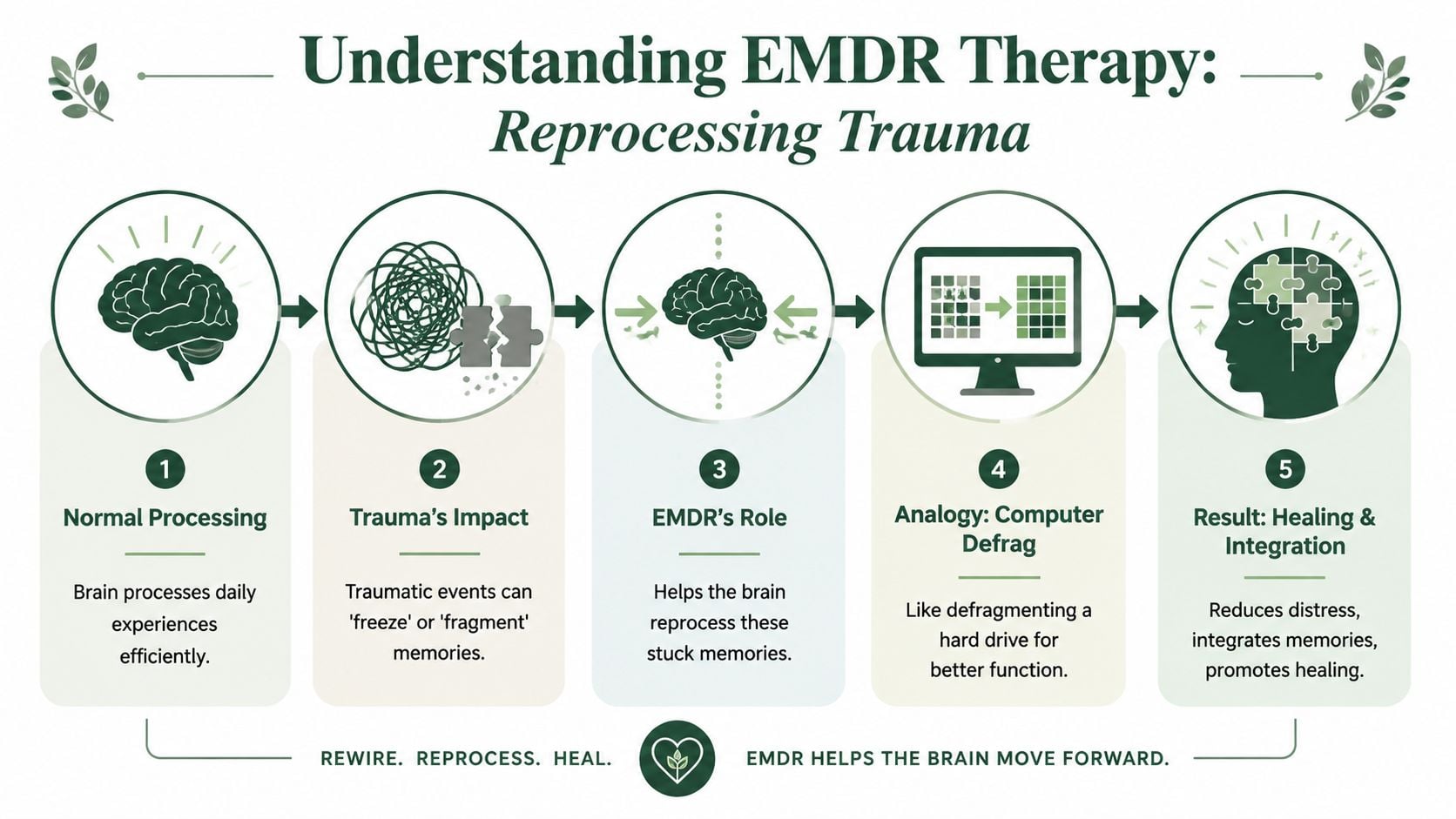
A useful way to understand EMDR is to think of the brain as a filing system. Most experiences get sorted, stored, and connected to other memories without much trouble. Trauma doesn't always get filed correctly. It can stay “live,” with the original fear, shame, helplessness, or bodily alarm attached.
That's why an old memory can feel current. The event is over, but the nervous system still reacts as if it isn't.
The basic idea behind reprocessing
EMDR uses bilateral stimulation, often side-to-side eye movements, alternating taps, or tones, while a person briefly focuses on a target memory. The goal isn't distraction. The goal is to help the brain do the processing it didn't complete at the time of the trauma.
A common analogy is a computer with a corrupted file. The file is still there, but it keeps freezing the system whenever it opens. EMDR helps the brain reconsolidate that memory so it becomes part of the past rather than an active threat in the present.
According to this clinical summary of EMDR's eight-phase protocol and session targets, EMDR typically uses 20 to 30 sets of side-to-side eye movements or alternating taps, distress is tracked with the Subjective Units of Disturbance Scale (SUDS, 0 to 10) and the Validity of Cognition (VOC, 1 to 7), and for single-incident trauma 80% of clients achieve the target outcome in 6 to 12 sessions.
What bilateral stimulation is actually doing
People often hear “eye movements” and assume EMDR is strange or theatrical. In practice, it's usually simple and calm. The therapist may move a hand back and forth, use alternating taps, or use audio tones.
What matters is function. Bilateral stimulation appears to support the brain's natural information processing, often described as similar to what happens during REM sleep. Instead of getting stuck in the emotional charge of the memory, the person can begin to notice shifts such as:
- Less intensity: The memory feels farther away.
- More accurate beliefs: “I'm powerless” may change into “I survived” or “I'm safe now.”
- Reduced body alarm: Tightness in the chest, nausea, shaking, or dread often decrease.
Practical rule: EMDR works best when it's paced well. Good therapy doesn't flood the client. It helps the client process without tipping into overwhelm.
Why this feels different from regular talk therapy
Traditional talk therapy can be valuable, but trauma often lives in images, body sensations, and automatic reactions. EMDR directly works with those pieces. A person doesn't need to deliver a perfect narrative for it to work. They need a trained clinician, a clear target, and enough stability to process safely.
That combination is a big reason people search for emdr therapy near me when they're tired of understanding their problem intellectually but still feeling it physically.
Who Can Benefit From EMDR Therapy
Many people associate EMDR only with combat trauma or severe accidents. It can help there, but that's too narrow. In practice, EMDR may be considered when a person's present-day symptoms are being driven by unresolved earlier experiences.
That can include obvious trauma, but also repeated emotional injuries, chaotic relationships, grief, shame, panic responses, and patterns that seem irrational until the underlying memory network is identified.

Common reasons someone may be a fit
EMDR may be appropriate for people dealing with:
- Post-traumatic stress symptoms: Nightmares, hypervigilance, flashbacks, or sudden emotional flooding.
- Complex trauma: Long-term exposure to instability, criticism, abuse, neglect, or betrayal.
- Anxiety and panic: Especially when reactions seem tied to earlier experiences rather than only current stress.
- Depressive patterns with trauma roots: Persistent shame, hopelessness, or self-blame can be linked to unresolved memory networks.
- Phobias and intense avoidance: Some fears are maintained by past experiences the brain never integrated.
A growing number of people also ask about EMDR when addiction is part of the picture. That's an important question, because trauma and substance use often reinforce each other.
Why EMDR matters in dual-diagnosis care
Some people use substances to sleep, shut down intrusive memories, numb shame, or stop the body from feeling constantly activated. If treatment only focuses on stopping the substance and doesn't treat the trauma that keeps driving it, relapse risk often remains high.
A summary of EMDR for addiction and trauma is helpful here. The broader evidence matters too. A 2023 meta-analysis found EMDR significantly reduced PTSD symptoms in people with substance use disorders and lowered craving intensity by 35% post-treatment. The same source notes that 45% of US adults in recovery have untreated trauma, while only 18% access integrated care, which shows why dual-diagnosis treatment is such a critical gap in care, according to this review of EMDR's role in substance use treatment.
Trade-offs become apparent. EMDR can be powerful, but it usually works best in a setting where the person also has support for sobriety, emotional regulation, relapse prevention, psychiatric needs, and daily functioning. Trauma processing without enough support can be mistimed. Addiction treatment without trauma care can be incomplete.
When integrated care tends to work better
A combined approach is often stronger when someone has:
| Situation | Why integrated care helps |
|---|---|
| Early recovery with strong triggers | The person needs coping tools and structure while trauma work begins |
| Repeated relapse after “good insight” | Insight alone may not resolve trauma-linked cravings |
| Trauma plus anxiety or depression | Treatment needs to address more than one symptom cluster |
| Shame after substance use | EMDR can target the emotional material that keeps the cycle going |
For readers comparing options beyond Massachusetts, this directory of integrative PTSD specialists in Philadelphia shows the same broader trend toward combined care rather than isolated symptom treatment.
The right question isn't “Does EMDR help trauma?” It's “Does the treatment setting also support sobriety, safety, and stabilization while trauma is being processed?”
A Step-by-Step Look Inside an EMDR Session
People are often less afraid of EMDR once they know what happens in the room. The process is structured. It doesn't start with diving headfirst into the worst memory. A trained clinician prepares the person first.
How the session sequence usually feels
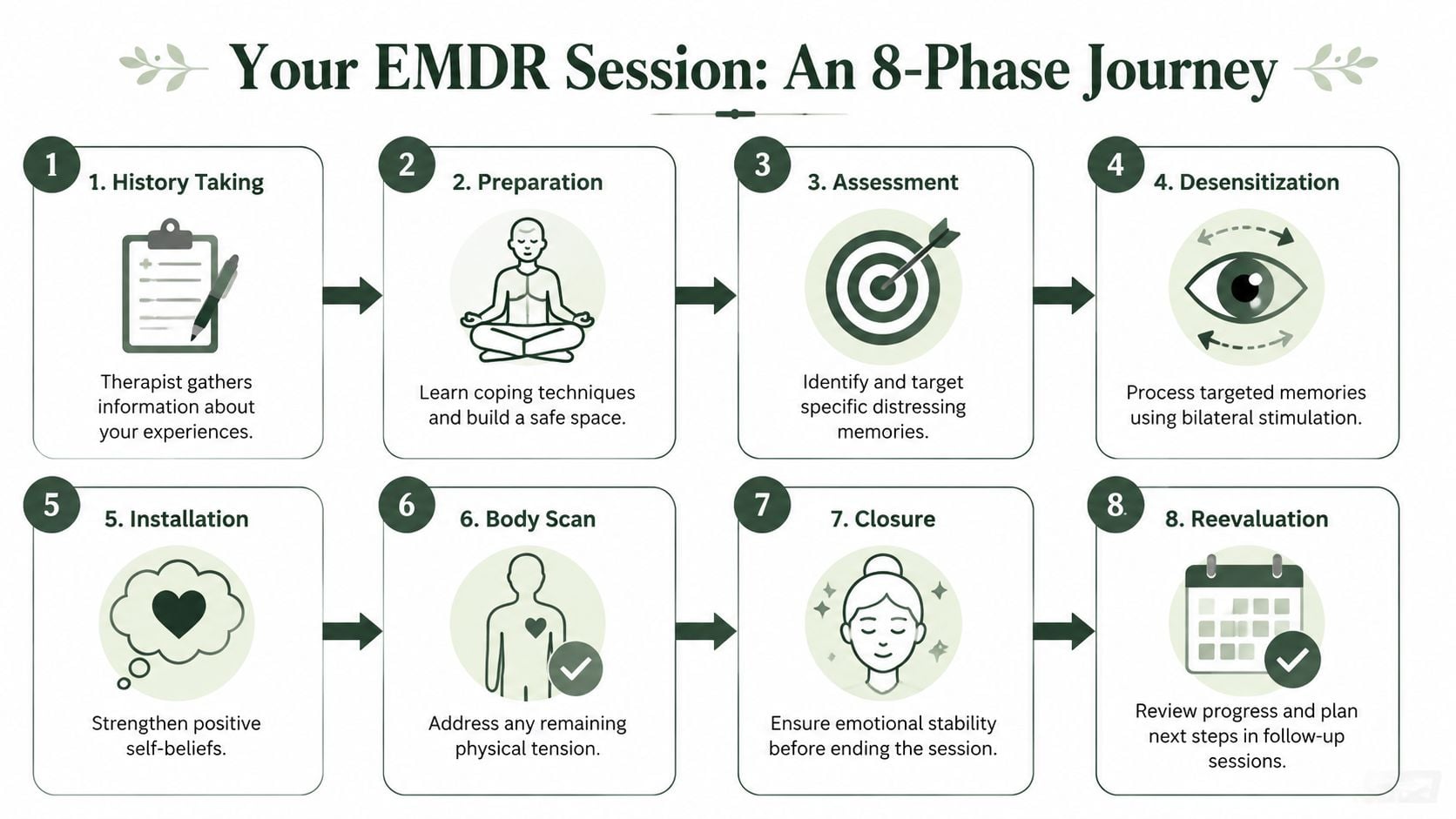
The early phase is about history and preparation. The therapist learns what happened, what symptoms are showing up now, and which memories, beliefs, or body responses seem most connected to current distress. The person also learns grounding tools, containment skills, and ways to settle after difficult material comes up.
Then comes assessment. A target memory is chosen. The therapist helps identify the image, the negative belief attached to it, the emotions, and where the distress shows up in the body. This is focused work, not random conversation.
What happens during processing
In the desensitization phase, the person brings the target memory to mind while following bilateral stimulation. After a short set, the therapist asks what the person notices. That might be an image, a thought, a body sensation, or an emotional shift.
The process continues in brief sets. Some people notice the memory changing. Others notice related memories surfacing. Many report that the same event begins to feel less charged and more distant.
According to this overview of Phase 4 and EMDR's trauma-processing mechanism, during desensitization clients focus on a traumatic memory's negative cognition while engaging in bilateral stimulation, which activates theta-band synchronization between brain hemispheres and promotes adaptive resolution of unprocessed memories. That same source reports an effect size of d = 1.22 for PTSD, described there as the largest among trauma therapies, and notes that the non-verbal nature of EMDR can help people who struggle to put feelings into words, which is common in substance use populations.
The rest of the eight phases
The later phases matter just as much as the processing itself:
- Installation: The therapist helps strengthen a more adaptive belief, such as “I'm safe now” or “I can protect myself.”
- Body scan: Residual tension gets checked, because trauma often remains in the body after the story changes.
- Closure: The session ends with enough stability for the person to return to daily life safely.
- Reevaluation: At the next session, the therapist checks what held, what shifted, and what still needs work.
Some sessions feel lighter right away. Others stir up material for a day or two before relief becomes clear. That doesn't automatically mean the treatment is going badly.
What tends not to work
A few common mistakes can get in the way:
- Starting too fast: If the person hasn't built enough coping capacity, processing can feel destabilizing.
- Treating EMDR like a script: Good clinicians follow the model, but they also pace it to the individual.
- Ignoring the body: Trauma isn't only a story. Physical reactions often signal what still needs attention.
When people look for emdr therapy near me, they're not just looking for someone who knows the technique. They're looking for someone who knows when to slow down, when to continue, and how to hold the larger treatment picture together.
The Scientific Proof Behind EMDRs Success
EMDR sometimes gets misunderstood because the name sounds unusual. The evidence base is the reason it has lasted. This is not fringe care.

What major organizations recognized
The most important point is simple. EMDR earned acceptance through research, not branding.
As outlined in this review of evidence-based trauma therapy and EMDR recognition, EMDR was developed in 1987 by Dr. Francine Shapiro, was designated by the APA as an effective treatment for PTSD by 1995, and was endorsed by the WHO as a first-line therapy for PTSD in 2013.
What the research shows
The same body of evidence includes a 2013 meta-analysis of 26 randomized controlled trials that found EMDR significantly more effective than no-treatment and comparable to or exceeding CBT for PTSD symptom reduction. That matters because randomized trials remain one of the clearest ways to evaluate whether a treatment produces meaningful change.
Another point often overlooked is how broadly EMDR has spread in clinical practice. According to the same source, more than 150,000 clinicians worldwide had been trained through EMDRIA by 2023. That doesn't prove quality by itself, but it does show that EMDR has moved far beyond a niche intervention.
Why evidence still needs judgment
Research support doesn't mean EMDR is identical for every person. A therapy can be well validated and still require good clinical timing. For example, someone in early recovery from substance use may need stabilization, structure, and psychiatric support before deeper trauma processing begins.
Strong evidence answers “Can this work?” Clinical skill answers “Is this the right time, pace, and setting?”
That distinction is important for anyone in Massachusetts looking for care that addresses more than one problem at once. A treatment can be scientifically sound, but it still has to be delivered in a way that fits the person's nervous system, substance use history, and support needs.
Finding the Right EMDR Therapist in Massachusetts
Not every therapist who mentions trauma treatment has advanced EMDR training. And not every EMDR therapist is equipped to work with addiction, OCD, dissociation, or complex co-occurring disorders. The search should be practical, not just hopeful.

What to check before booking
A solid first screen includes the following:
- Training and certification: Ask whether the clinician has formal EMDR training and whether they regularly use the full protocol rather than borrowing isolated techniques.
- Experience with your specific issues: Trauma tied to alcohol use, opioids, compulsions, or chronic relapse often needs different pacing than single-incident trauma.
- Setting and support: Some people do well in standard outpatient therapy. Others need a higher level of care so trauma work doesn't outpace their stability.
- Clear explanation of treatment: A good clinician should be able to explain how sessions work in plain language.
For people who want a broader framework for evaluating fit, this guide on how to find a therapist is a useful starting point.
Questions worth asking on the first call
A first phone call doesn't need to be long. It should answer the questions that shape safety and fit.
| Question | Why it matters |
|---|---|
| Do you treat trauma and substance use together? | Many people need both addressed at the same time |
| How do you decide when someone is ready for EMDR? | Timing affects safety and outcomes |
| What happens if EMDR brings up intense emotions between sessions? | Good care includes a plan for support |
| Do you coordinate care across levels of treatment? | Complex cases usually improve with continuity |
What often separates strong care from weak care
The biggest difference is whether the clinician sees EMDR as one tool inside a larger treatment plan. Trauma rarely happens in a vacuum. A person may also be dealing with cravings, family strain, panic, depression, obsessive symptoms, or unstable routines.
What doesn't help is a narrow approach that focuses on only one layer. A person may technically receive EMDR but still struggle because sleep, relapse triggers, medications, or emotional regulation were never addressed alongside it.
The best trauma treatment usually feels organized. The client knows the plan, understands the pace, and isn't left alone to manage the fallout of difficult work.
For Massachusetts residents, local treatment programs are especially relevant. A center that can provide evaluation, dual-diagnosis treatment, outpatient support, and ongoing trauma work removes a lot of the fragmentation that slows recovery. That kind of continuity is especially important when someone is trying to heal from trauma without losing ground in sobriety, work, parenting, or daily functioning.
Common Questions About Starting EMDR Therapy
Is EMDR covered by insurance
Coverage depends on the plan, the level of care, and whether services are in network or out of network. The practical move is to verify benefits before treatment starts. People who need addiction and trauma care together should also ask whether dual-diagnosis treatment, outpatient services, or higher levels of care are included.
How is EMDR different from talk therapy
Talk therapy often focuses on insight, patterns, and verbal processing. EMDR is more targeted. It works directly with distressing memories, negative beliefs, and body responses using bilateral stimulation within a structured protocol. Many people prefer that it doesn't require endless retelling to produce change.
Can EMDR help with OCD
In some cases, yes, especially when obsessive symptoms are tied to unresolved trauma. A 2025 multi-center RCT found that combining EMDR with ERP reduced OCD symptoms by 52% compared with 38% for ERP alone, and this approach was described as especially useful for the 67% of dual-diagnosis OCD cases in which intrusions are rooted in unresolved trauma, according to this summary of EMDR and OCD treatment research.
Is EMDR too intense if someone is newly sober
Not automatically. But timing matters. Some people benefit from starting with stabilization, coping skills, and relapse prevention before deeper processing begins. That's why integrated treatment is often the safest option for trauma and addiction together.
A person searching for emdr therapy near me is usually looking for relief, but also for clarity. EMDR offers both when it's delivered thoughtfully, paced correctly, and placed inside a treatment plan that addresses the full picture.
If trauma, addiction, anxiety, or OCD symptoms are still shaping daily life, Paramount Recovery Centers offers Massachusetts clients a practical path forward with integrated, evidence-based care. Their team provides dual-diagnosis treatment, trauma-informed support, and help navigating next steps, including insurance verification and level-of-care guidance. To speak with someone confidentially today, call (888) 388-8660.
