

Sleep may be broken. Concentration may disappear at work. A crowded store, a slammed door, a difficult conversation, or a quiet night alone may bring the past back into the present so fast that it feels impossible to trust the body or the mind. Many adults live in that cycle for far too long, especially when trauma and substance use start feeding each other.
That stuck feeling is painful, but it isn’t proof that healing is out of reach. Effective treatment exists. Evidence based trauma therapy means treatment that has been tested carefully, refined over time, and shown to help people reduce trauma symptoms in a structured way. It gives recovery a method instead of guesswork.
Healing That Works Your Guide to Evidence-Based Trauma Therapy
Trauma doesn’t always look dramatic from the outside. Sometimes it looks like isolation, irritability, numbness, panic, sleep problems, shame, or the need to stay busy so difficult memories never have a chance to surface. It can also look like drinking or drug use that started as a way to calm the nervous system and slowly became another source of suffering.
Trauma is also common. Nearly 90% of adults in the United States have reported exposure to traumatic events, and globally the World Health Organization reports that 70.4% of respondents across 24 countries endorsed lifetime traumas according to The Permanente Journal review. The need for real treatment is not rare, unusual, or limited to one type of person.
What people usually want to know first
People searching for help aren’t asking for a theory lesson. They want clear answers to practical questions:
- Will treatment help: They want something more dependable than “just talk about it.”
- Will anyone understand both trauma and addiction: Many people have tried care that focused on one problem and ignored the other.
- Will they be pushed too hard: Fear of being overwhelmed keeps many people from starting.
Those questions are reasonable. Good trauma care answers them directly.
Evidence based trauma therapy works best when treatment is structured, paced, and matched to the person’s symptoms, safety needs, and recovery goals.
What this kind of care offers
A strong trauma treatment plan usually includes several elements working together:
- A careful assessment that looks at trauma symptoms, mental health, substance use, functioning, and readiness.
- A named therapy model such as CPT, PE, TF-CBT, or EMDR, rather than vague supportive counseling alone.
- Clear goals so progress can be measured in daily life, not just discussed in session.
- A plan for avoidance because trauma often makes people pull back right when help matters most.
For people in Massachusetts who need both trauma treatment and substance use care, that level of structure matters. Recovery is more stable when clinicians address the trauma underneath the symptoms instead of only reacting to the crisis on the surface.
What Evidence-Based Really Means for Trauma Healing
Evidence based treatment isn’t a marketing phrase. It means a therapy has been studied closely and has earned its place through repeated testing. In trauma work, that matters because trauma treatment has to do two things at once. It has to be effective, and it has to be delivered safely.
Blueprint, not guesswork
A useful comparison is a bridge. An engineer doesn’t build a bridge by intuition alone. The design is based on tested principles, known materials, stress limits, and repeated inspection. Trauma therapy should work the same way.
When treatment is evidence based, the clinician isn’t inventing a process session by session. The work follows a model that has been evaluated, taught, supervised, and improved. That gives patients something essential after trauma: predictability.
What separates it from general talk therapy
Supportive therapy can be helpful. It can reduce isolation, offer validation, and create space to speak openly. But trauma symptoms often stay stuck when treatment never directly addresses avoidance, distorted beliefs, fear conditioning, or trauma-related triggers.
Evidence based trauma therapy usually includes the following:
- A clear mechanism: The treatment targets a known trauma process, such as avoidance or trauma-linked beliefs.
- A defined structure: Sessions have a purpose rather than drifting wherever distress leads that day.
- Specific skills or exercises: Patients practice tools between sessions, not only during them.
- A planned course of care: Treatment has direction, even when pacing is flexible.
Practical rule: If a provider can’t explain how a therapy works, what it targets, and how progress is evaluated, the care may be too vague for trauma recovery.
Why training matters
The model matters, but training matters too. A therapy isn’t evidence based solely because a provider uses the name. Clinicians need instruction, supervision, and ongoing learning to deliver trauma treatment well. That’s one reason professional development remains important in behavioral health. For readers curious about how clinicians maintain structured training standards, Continuing Education Units (CEUs) are part of how many licensed professionals keep building competence after formal schooling.
That matters in trauma care because small choices affect outcomes. Timing, pacing, preparation, safety planning, and how a clinician responds to shutdown or avoidance can change whether a person stays engaged or drops out.
What patients should expect
A patient should expect more than empathy alone. They should expect a treatment plan that makes clinical sense.
That includes an explanation of why a certain method is being recommended, what sessions may involve, what to do if symptoms rise temporarily, and how the treatment fits with addiction recovery if substances are part of the picture. Good care doesn’t promise comfort every step of the way. It offers a path that is thoughtful, tested, and built for healing.
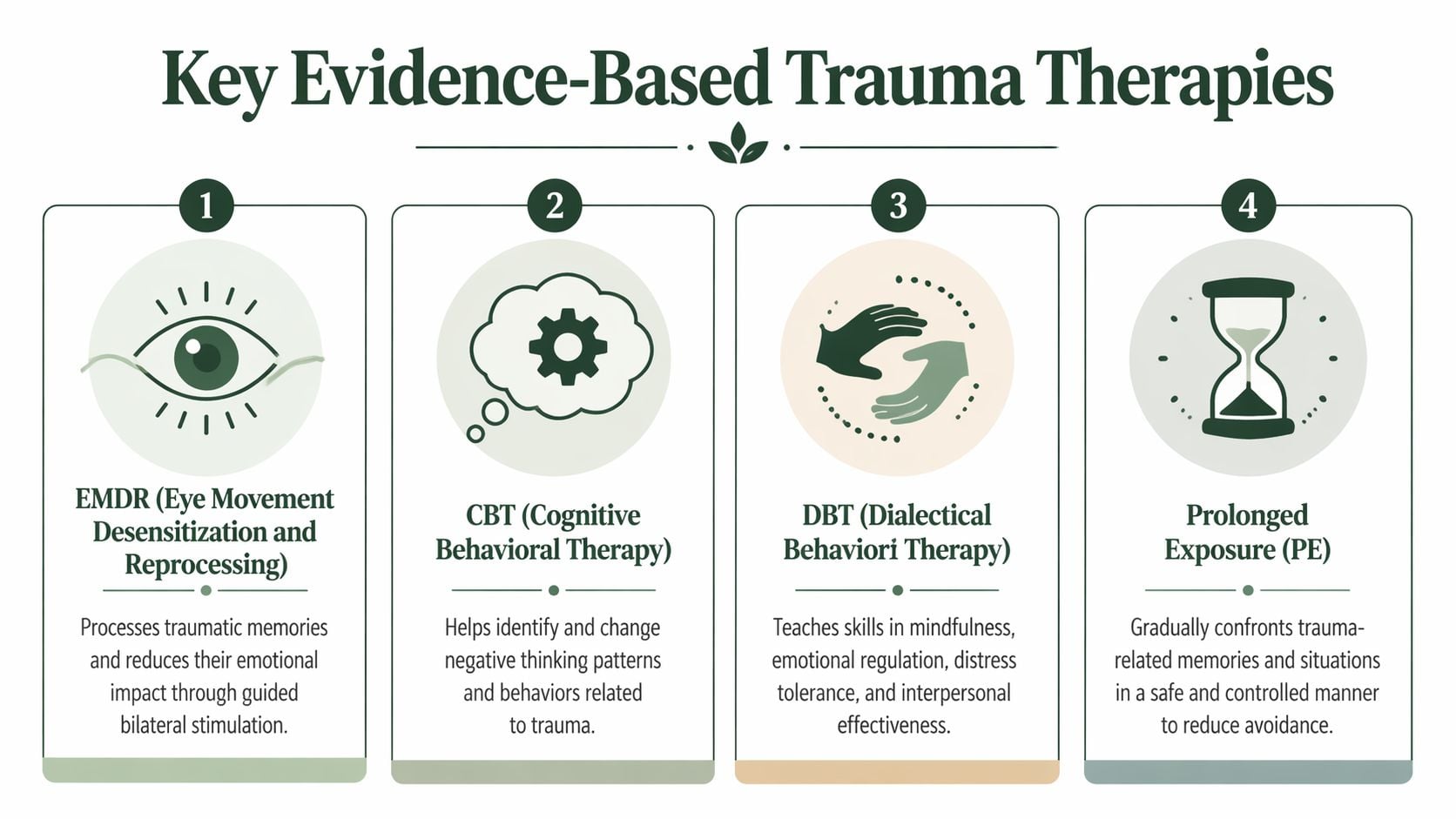
Key Trauma Therapies with Proven Results
The strongest trauma plans don’t start with “Which therapy is trendy?” They start with “What is maintaining this person’s symptoms?” Some people are dominated by avoidance. Others are trapped by guilt, shame, or beliefs about danger. Some need more preparation and stabilization before doing deeper trauma processing. The treatment should fit the pattern.
Cognitive Processing Therapy
Cognitive Processing Therapy, often called CPT, focuses on how trauma changes beliefs. After trauma, people may become fixed in thoughts such as “It was my fault,” “No one can be trusted,” or “I’m never safe.” Those beliefs can feel like facts because they were shaped under extreme stress.
CPT helps patients identify those stuck points, examine them carefully, and replace them with thinking that is more accurate and less driven by trauma. This is not forced positivity. It is disciplined cognitive work.
For readers who want a plain-language look at the model itself, this overview of Cognitive Processing Therapy (CPT) gives useful background on the approach and its training framework.
CPT is often a good fit when shame, guilt, anger, and rigid beliefs keep symptoms active. It can be especially helpful for people who need a clear structure and want to understand why they react the way they do.
Prolonged Exposure therapy
Prolonged Exposure therapy, or PE, targets avoidance directly. PTSD often survives because the person learns to avoid reminders, memories, emotions, situations, or sensations connected to the trauma. That avoidance lowers distress in the short term, but it keeps fear in place.
PE is designed to interrupt that pattern. It typically includes revisiting trauma memories in a guided way and gradually approaching safe situations that the person has been avoiding. According to the APA overview of updated PTSD treatment guidelines, PE typically consists of approximately 12 sessions of 90-minute duration and has shown greater reduction in PTSD symptoms than non-trauma-focused therapies, with treated individuals less likely to meet PTSD diagnostic criteria after treatment.
That doesn’t mean PE is right for everyone at every moment. Some people need more preparation first. Others do better with a cognitive approach. But when avoidance is the engine of suffering, PE can be a very strong option.
A common misunderstanding is that PE means flooding someone with pain. Good PE is paced, collaborative, and highly structured.
Trauma-Focused Cognitive Behavioral Therapy
TF-CBT is best known for children and adolescents, but the broader trauma-focused CBT family has a strong role in trauma care more generally. The core idea is practical. Trauma affects thoughts, emotions, behavior, and the body all at once, so treatment addresses all of them.
The verified data notes that TF-CBT is often delivered in 12 to 20 sessions and has shown effectiveness across youth and adults, including people with complex trauma. It can reduce PTSD symptoms while also helping with depression, behavior problems, and emotional regulation.
This model is often useful when trauma symptoms are mixed with anxiety, mood symptoms, family strain, or difficulty managing daily routines. It gives patients both processing and coping tools.
EMDR
EMDR, or Eye Movement Desensitization and Reprocessing, is widely used in trauma treatment and is part of many specialized trauma programs. In plain terms, EMDR helps people process disturbing memories so those memories become less emotionally overwhelming and less disruptive in everyday life.
Some patients prefer EMDR because it can feel less verbally exhausting than therapies built around extended discussion of trauma narratives. Others respond better to methods that lean more heavily on direct cognitive work or exposure. The key point is that EMDR should be delivered within a thoughtful treatment plan, not treated as a stand-alone quick fix.
Skills-based supports that often matter
A person may need more than one therapy element to recover well, especially when trauma overlaps with addiction, depression, panic, or unstable relationships. Some of the most useful additions include:
- CBT skills work: Patients learn how triggers, thoughts, emotions, and behavior connect. A deeper explanation appears in Paramount’s guide to cognitive behavioral therapy.
- DBT-informed skills: Distress tolerance, emotional regulation, mindfulness, and interpersonal effectiveness help patients stay in treatment when emotions spike.
- Motivational enhancement: This helps when ambivalence, shame, or fear make it hard to engage openly.
- Relapse prevention planning: Trauma cues often overlap with cravings, so both have to be mapped together.
Comparing Evidence-Based Trauma Therapies
| Therapy | How It Works | Best For | Typical Duration |
|---|---|---|---|
| CPT | Examines and updates trauma-driven beliefs and stuck points | Guilt, shame, self-blame, negative beliefs about safety or trust | Structured course, often within the evidence-based brief therapy range |
| PE | Gradually reduces avoidance through imaginal and in vivo exposure | PTSD maintained by avoidance, fear, and trauma reminders | Approximately 12 sessions of 90 minutes |
| TF-CBT | Combines coping skills, cognitive work, and trauma processing | Complex trauma, emotional regulation difficulties, mixed trauma and mood symptoms | 12 to 20 sessions |
| EMDR | Processes traumatic memories with structured bilateral stimulation | People who benefit from less verbally intensive trauma processing or integrated trauma work | Varies by treatment plan and symptom complexity |
How clinicians choose among them
Clinicians usually look at several decision points rather than choosing by label alone:
- Main maintaining factor: If avoidance dominates, PE may make sense. If distorted beliefs dominate, CPT may be the better fit.
- Readiness and stability: A patient with active substance use, severe dissociation, or poor sleep may need stabilization first.
- Treatment setting: Outpatient, day treatment, and dual-diagnosis settings call for different pacing.
- Patient preference: Engagement improves when the patient understands and accepts the rationale.
No single model solves every presentation. The strongest programs use proven therapies as tools inside a broader plan.
The Dual Diagnosis Challenge Trauma and Substance Use
Trauma and substance use often become intertwined for understandable reasons. Alcohol, opioids, stimulants, cannabis, or sedatives may begin as a way to sleep, shut off panic, numb shame, blunt intrusive memories, or get through social situations that feel unsafe. What starts as coping can become dependence, and dependence then creates new instability that makes trauma symptoms worse.
That cycle is why treatment fails when care is split into silos. If a program treats addiction but never addresses trauma, the person may leave sober but still overwhelmed by the same triggers that fueled use. If a therapist focuses on trauma but ignores ongoing substance use, the person may struggle to stay regulated enough to benefit from the work.
Why integrated treatment matters
Dual diagnosis care brings both problems into the same plan. The clinician doesn’t treat trauma as a side issue and doesn’t treat substance use as mere bad behavior. Both are clinical realities affecting the same nervous system.
An integrated plan often includes:
- Trigger mapping: Identifying where trauma reminders and cravings overlap.
- Sequencing decisions: Determining when a person needs detox coordination, stabilization, medication support, or trauma processing.
- Shared goals across the team: Therapists, prescribers, and recovery staff work from one plan rather than separate agendas.
- Relapse prevention tied to trauma cues: The patient learns how flashbacks, shame spirals, conflict, or loneliness can activate use.
What doesn’t work well
Several patterns tend to undermine progress:
- Treating substance use as the only problem. That approach often misses the reason use became reinforcing.
- Starting trauma work without safety planning. If the nervous system is overwhelmed, engagement often drops fast.
- Using generic coping advice alone. Patients need targeted interventions, not just encouragement to “open up.”
For Massachusetts residents seeking both mental health and addiction care, the treatment model should be integrated from the start. A practical overview of that approach appears in this explanation of dual diagnosis treatment effectiveness.
When trauma and addiction drive each other, recovery gets stronger when one team treats both at the same time.
One clinical recommendation, stated plainly
A specialized program can combine evidence-based trauma therapies, addiction treatment, medication management, group work, and family support under one roof. Paramount Recovery Centers provides that kind of dual-diagnosis structure in Massachusetts, including trauma-informed and evidence-based services for adults whose substance use and mental health symptoms are connected.
How Trauma Therapy Is Personalized for Your Recovery
Personalized care isn’t about making treatment softer. It’s about making treatment precise enough to work. Two people may both carry trauma histories and substance use problems, yet need very different plans based on their symptoms, medical needs, relationships, and capacity to tolerate distress.
That need for precision is one reason specialized teams matter. The available evidence notes that specialized clinicians are scarce even in Europe and the U.S., with limited infrastructure for trauma-focused training, as discussed in the ISTSS article on access to trauma interventions. In practice, that means a strong treatment setting needs more than good intentions. It needs clinicians who can match the method to the person.
Individual therapy and group therapy do different jobs
Individual sessions give patients privacy for detailed trauma formulation, sensitive history, and direct work on beliefs, memories, and avoidance. This is often where pacing decisions are made carefully.
Group therapy serves a different function. It reduces isolation, challenges shame, and lets patients practice honesty, boundaries, and emotional regulation with other people present. For many trauma survivors, that social repair is part of the healing itself.
A balanced plan may use both because they solve different problems.
Gender-responsive care can improve safety and honesty
Men and women often arrive with different barriers to disclosure, different social pressures, and different trauma-related themes. Some men minimize vulnerability until symptoms become severe. Some women carry trauma histories shaped by coercion, caregiving burdens, or fear of not being believed. Those patterns don’t define every person, but they matter clinically.
Gender-responsive programming can help by offering:
- A safer discussion environment: Patients may speak more openly when they feel less socially exposed.
- More relevant clinical examples: Groups can address common relational and family dynamics in a focused way.
- Better pacing for disclosure: Patients don’t all build trust the same way.
The full plan usually includes more than one track
A personalized recovery plan often pulls together several treatment layers at once:
- Trauma-focused therapy for the core PTSD symptoms
- Addiction treatment for cravings, relapse risk, and recovery routines
- Psychiatric support when mood, sleep, or anxiety symptoms interfere with treatment
- Family work when the home environment affects safety or recovery
- Aftercare planning so progress doesn’t end when the highest level of care ends
The right trauma plan doesn’t ask, “What therapy is everyone else doing?” It asks, “What does this person need to stay engaged and keep moving forward?”
That’s the difference between a generic program and one that can hold complexity without losing direction.
Begin Your Recovery at Paramount Recovery Centers
Starting treatment is often hardest before the first call. Many people worry they’ll be judged, rushed, or pushed to describe painful experiences before trust exists. That fear is common in trauma care, and it should be taken seriously.
Patient avoidance is a core symptom of PTSD and can block treatment engagement. The verified data also notes that effective care overcomes this by building trust and using motivational techniques so therapy matches a client’s readiness for change, as described in the Blueprint discussion of evidence-based trauma treatment options.

What the first step usually looks like
A strong admissions process should feel direct and calm. The first conversation usually focuses on what is happening now, not on forcing a complete trauma account immediately.
That early process often includes:
- Confidential discussion: The admissions or clinical team asks about symptoms, substance use, safety concerns, and immediate needs.
- Level-of-care planning: The team determines whether the person needs detox coordination, inpatient care, day treatment, outpatient treatment, or a combination over time.
- Treatment matching: Clinicians identify which evidence-based approaches make sense first.
- Insurance and logistics review: Practical barriers are addressed early so care can begin with less delay.
What people often fear, and what good care does instead
Many patients fear they’ll be forced into exposure work before they’re ready. Good trauma treatment doesn’t work that way. It explains the rationale, sets expectations, prepares the patient, and uses pacing that keeps the person engaged rather than flooded.
Others fear that asking for help means losing control. In a sound program, the opposite should happen. The patient gains a structured plan, a team that understands co-occurring conditions, and a clearer sense of what healing can look like.
For those considering more personalized clinical support, this overview of individual therapy in Massachusetts shows how one-on-one treatment can be built into a larger recovery plan.
Why action matters now
Trauma rarely improves through avoidance alone. Addiction rarely stabilizes when trauma keeps driving the nervous system back into fear, shame, numbness, or chaos. Waiting may feel safer in the short term, but it often gives both problems more room to grow.
A skilled treatment team can slow the process down where needed, speed it up where appropriate, and build a plan that addresses both trauma and substance use with real clinical structure. Your path to healing is one call away. Contact the team 24/7 at (888) 388-8660.
Frequently Asked Questions About Trauma Therapy
Will someone have to relive trauma over and over again
No. Evidence based trauma therapy is not the same as being pushed to repeatedly retell painful events without a purpose. Structured trauma treatment uses specific methods to reduce the power those memories hold. Some therapies involve talking more directly about the trauma, while others focus more on beliefs, coping skills, or guided processing. The pace should be clinically sound and emotionally manageable.
How can someone know if what happened was bad enough for therapy
If an experience still affects sleep, safety, mood, relationships, substance use, work, or day-to-day functioning, it’s worth bringing into treatment. Trauma isn’t defined only by one dramatic event. Many people struggle after repeated stress, childhood adversity, violence, loss, neglect, or other overwhelming experiences. The impact matters.
Is evidence based trauma therapy covered by insurance
Coverage depends on the plan, level of care, and clinical needs. Many treatment centers verify benefits and explain options before admission. The fastest way to get a clear answer is to speak directly with an admissions team that can review the insurance details and recommended level of care.
What if someone wants help but isn’t ready to talk about everything
That’s common. Avoidance is part of trauma, not a sign that treatment can’t work. Good clinicians build safety and trust first, then help the person move forward in a way that is structured and realistic. Starting the conversation is often the hardest step.
If trauma, PTSD symptoms, and substance use are shaping daily life, Paramount Recovery Centers offers a place to begin with confidential support, evidence-based care, and treatment planning built around the person’s actual needs. Call (888) 388-8660 to speak with the admissions team and take the next step toward recovery.
