
When a family starts searching for help, the pattern is often the same. A son stops sleeping, starts drinking more, and becomes impossible to reach. A spouse quits opioids for a few days, then panic and depression crash in and the use starts again. A daughter looks “fine” at work, then unravels at home with mood swings, isolation, and secret substance use. The family keeps asking the same question: is this addiction, is this mental health, or is it both?
For many people, it’s both.
That’s why dual diagnosis treatment programs matter so much in Massachusetts and everywhere else. They’re built for people who aren’t dealing with one clean, separate problem. They’re dealing with a knot of symptoms, behavior, trauma, cravings, fear, and often shame. Untangling that knot takes coordinated care, not guesswork.
Why Integrated Treatment is Essential for Recovery
A person with dual diagnosis isn’t failing treatment because they “don’t want it enough.” Often, they’ve been treated in pieces. One provider focuses on substance use. Another focuses on anxiety, depression, trauma, bipolar symptoms, or obsessive thoughts. The person leaves with partial relief, then relapses because the untreated condition keeps pushing the other one forward.

Two problems feeding each other
Dual diagnosis means a substance use disorder and a mental health disorder are happening at the same time. In real life, that can look like someone drinking to quiet panic, misusing stimulants while cycling through depression, or using opioids to numb trauma symptoms. The substance may seem to help for a few hours. Then sleep gets worse, mood gets worse, judgment gets worse, and the original psychiatric symptoms return with more force.
That’s why treating only one side rarely holds.
A person can stop using for a short period, but if severe anxiety, trauma triggers, or unstable mood remain untreated, the urge to self-medicate often comes roaring back. The reverse is also true. A person can start therapy for depression or PTSD, but if substance use continues unchecked, progress stays fragile.
Practical rule: If a program can’t explain how it treats addiction and mental health together, it’s not designed for true dual diagnosis care.
Why integrated care changes the outcome
The need for this approach isn’t rare. In 2014, approximately 20.2 million adults in the United States had a substance use disorder, and 7.9 million of them, nearly 39%, also had a co-occurring mental health disorder, according to National mental illness and substance use figures summarized here. That’s not a niche clinical issue. It’s a common reality.
Integrated treatment means one coordinated plan addresses detox needs, psychiatric symptoms, therapy goals, medication questions, family communication, and relapse prevention at the same time. The clinical team isn’t arguing over which problem came first. They’re addressing what’s keeping the person sick today.
For families in crisis, that shift matters. It replaces blame with a workable plan. It also helps explain why a loved one may have “tried treatment” before and still not gotten well. The issue may not have been effort. The issue may have been fit.
Common Co-Occurring Disorders and Their Symptoms
A family often calls after months of arguing about what the “real” problem is. Is it the drinking? The panic attacks? The shutdown after trauma? The answer is often both. In dual diagnosis care, the pattern matters as much as the individual symptoms, because the substance is usually doing a job for the person, even while it is making the overall condition worse.
That is why a careful intake at a quality program does more than list diagnoses. It looks at what the person uses, what they are trying to escape or control, when symptoms started, and how those symptoms change during periods of use, withdrawal, and sobriety. In Massachusetts, that level of sorting matters even more when families are trying to choose a gender-specific setting with the right clinical depth. Paramount Recovery Centers uses that kind of real-world assessment as the standard. The goal is to place a person where treatment fits the actual problem, not just the most visible one.
Anxiety and alcohol
This is a common pairing.
A person feels tense all day, dreads social situations, cannot quiet racing thoughts, or lies awake at night bracing for the next problem. Alcohol can bring fast relief. Then sleep gets lighter, the body rebounds with more anxiety, and the person starts needing alcohol not to feel good, but to feel less bad.
Common signs include:
- Constant overthinking: racing thoughts, dread, or a persistent sense that something bad is about to happen
- Avoidance: skipping work events, family gatherings, or routine responsibilities because anxiety feels unmanageable
- Using alcohol as a coping tool: drinking before bed, before social situations, or after stress to calm down
Families often mistake this for poor motivation or attitude. It is usually a cycle of untreated anxiety and short-term chemical relief.
Depression and opioids or sedatives
Depression can look quiet from the outside. The person may seem tired, detached, irritable, or uninterested in anything that used to matter. Opioids or sedatives can feel like relief because they numb emotional pain, slow the mind, and reduce distress for a few hours. Over time, mood often gets flatter, daily functioning slips, and the person may start using just to get through the day.
Watch for low energy, hopelessness, loss of interest, guilt, isolation, oversleeping or insomnia, and a growing need for pills or other substances to feel normal.
Trauma and polysubstance use
Trauma rarely shows up in a neat, single-symptom package. A person may use one substance to sleep, another to stay alert, and another to shut down flashbacks, panic, or hypervigilance. Families see erratic behavior. Clinicians usually see a nervous system stuck in survival mode.
When a loved one says, “Using is the only thing that helps,” treat that as clinical information. It points to pain that still needs direct treatment.
The National Institute on Drug Abuse explains that substance use and mental disorders often occur together, and one condition can affect the course of the other, which is why accurate assessment has to examine both at the same time. Review the agency’s overview of co-occurring substance use and mental disorders for a clear summary.
Bipolar symptoms, OCD, ADHD, and other combinations
Some combinations are harder for families to recognize because the symptoms can look like personality problems, immaturity, or defiance. Bipolar disorder may show up as impulsive spending, agitation, risky behavior, and stretches of very little sleep. OCD can drive repetitive rituals, mental checking, and severe distress that a person tries to quiet with substances. ADHD can add disorganization, emotional reactivity, and impulsive use that gets mistaken for lack of effort.
For families trying to make sense of emotional volatility, impulsivity, or overwhelm, resources on practical emotional regulation for ADHD can be useful alongside a formal clinical evaluation.
Diagnosis can take time. Early sobriety may uncover symptoms that were hidden by substance use, while heavy use can mimic psychiatric illness. That is one reason families should ask whether a program can reassess the picture over time and adjust care as the person stabilizes. If you are trying to understand how symptom severity and psychiatric needs affect placement, this guide on whether a full continuum of care for addiction recovery is needed will help clarify the next decision.
The practical takeaway is simple. If the symptoms keep feeding the substance use, and the substance use keeps intensifying the symptoms, your family is likely dealing with a dual diagnosis case that needs coordinated treatment, not guesswork.
The Full Continuum of Care for Dual Diagnosis
A family usually reaches this point after a rough stretch. Maybe there was an ER visit, a relapse after a short program, or a week when depression, panic, or mania made the substance use worse by the day. The question becomes practical very quickly. What level of care does this person need right now, and what should happen after that?
Families often use the word “rehab” as if it describes one setting. Dual diagnosis treatment works better as a sequence of settings, each with a clear job. The goal is to stabilize the person, treat the psychiatric symptoms and substance use together, and step down carefully so progress holds once daily life starts putting pressure on recovery again.
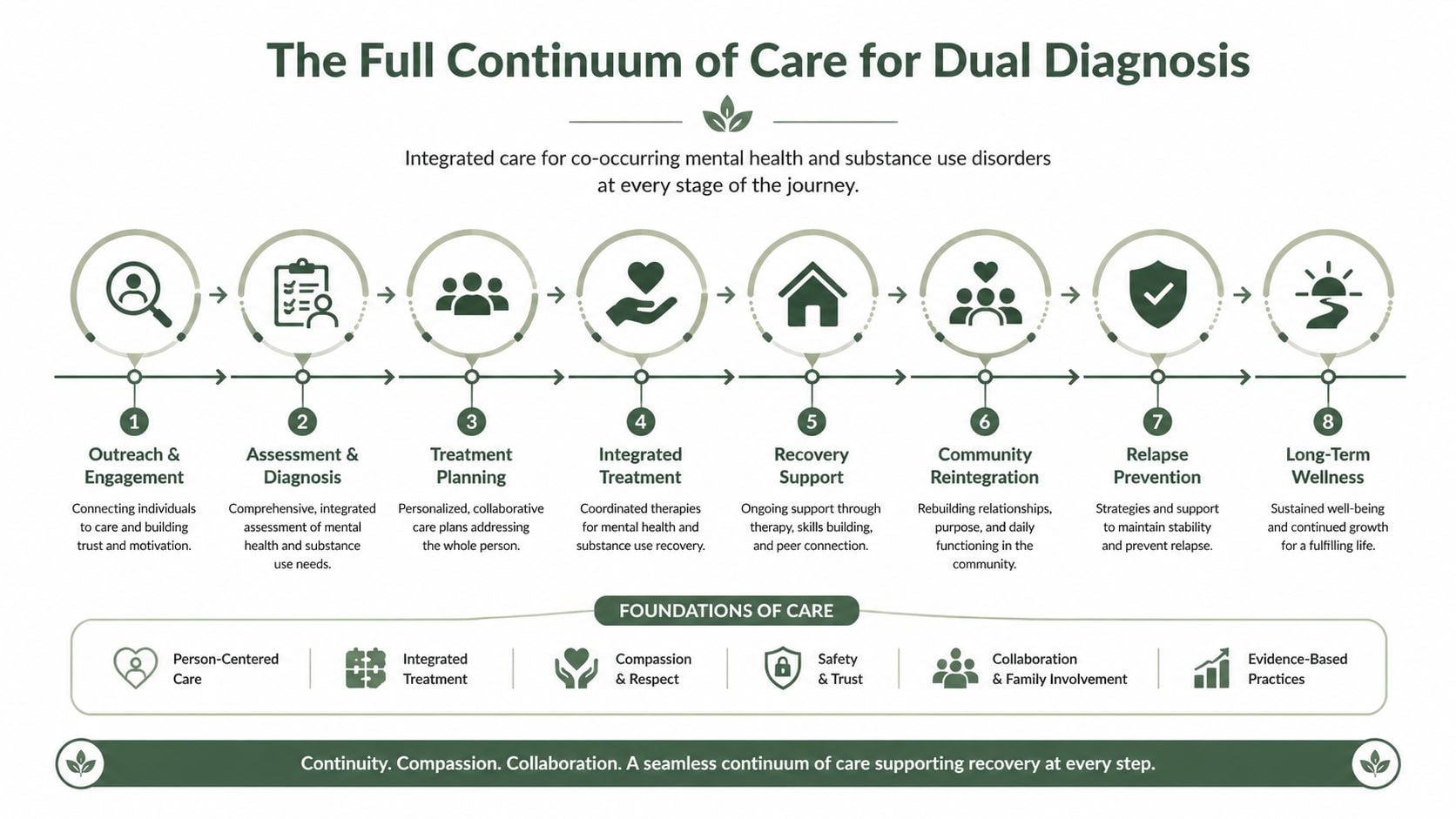
What each level of care is for
Placement should match current risk, symptom severity, and home stability. A person with withdrawal risk, suicidal thinking, or severe mood instability needs more support than someone who is medically stable and able to participate safely during the day.
| Level of care | Main purpose | Best fit |
|---|---|---|
| Detox placement | Safe withdrawal management and medical stabilization | Recent heavy use, withdrawal risk, unstable physical symptoms |
| Residential or inpatient | Intensive structure, psychiatric support, therapy, and daily accountability | High relapse risk, unsafe home setting, major symptom burden |
| PHP | Day treatment with strong clinical support while building real-world functioning | Needs high support but not overnight care |
| IOP | Continued therapy and skill practice with more flexibility | Stepping down from higher care or managing work and family demands |
| Outpatient | Ongoing individual, group, and medication follow-up | Greater stability with continued monitoring needed |
| Aftercare and alumni | Relapse prevention, connection, and long-term accountability | Anyone finishing formal treatment |
The right level is not always the least restrictive setting a person wants. It is the lowest level that can still keep the person safe, engaged, and clinically stable.
Why enough time in treatment matters
Families often ask for the shortest path because jobs, children, school, and insurance limits are real pressures. Those concerns should be addressed directly. They still do not change the clinical reality that dual diagnosis cases often need time.
Early recovery can be messy. Sleep has to normalize. Medications may need adjustment. Trauma work may need to wait until the person is more stable. A diagnosis that looked obvious during active use may look different after a few sober weeks. Short stays can start the process, but they may not be long enough to finish the first phase well.
A better question is whether the program gives treatment enough time to work.
One coordinated path reduces setbacks
Patients do worse when every step down means a new team, a new assessment, and a new treatment plan built from scratch. Important details get lost. Medication history gets oversimplified. Family patterns get missed. The patient gets tired of retelling painful facts to strangers.
Programs with a full range of care can reduce those breaks. Families who want to understand how levels fit together can review what a full continuum of care for addiction recovery includes. In Massachusetts, Paramount Recovery Centers offers detox coordination, inpatient treatment, PHP, IOP, outpatient care, aftercare, and gender-specific dual diagnosis programming. For many families, that means one clinical home base from the first phone call through the step-down process, which makes decisions clearer and handoffs smoother.
Gender-specific care also matters more than many families expect. Men and women often arrive with different trauma histories, relationship pressures, safety concerns, and barriers to honest group participation. In practice, the right setting can increase engagement, lower defensiveness, and help patients say what is actually happening.
If your family is trying to decide where to start, the next step is a clinical admissions call. A good program will ask about substance use, psychiatric symptoms, medications, safety risks, prior treatment, home environment, and insurance, then recommend the level of care that fits the current situation.
Evidence-Based Therapies That Drive Results
A strong program does more than provide a safe bed and a daily schedule. It uses therapies that target the mechanisms keeping a person stuck. In dual diagnosis treatment programs, the question isn’t just “what therapy is offered?” The better question is “what symptom or behavior does this therapy help change?”
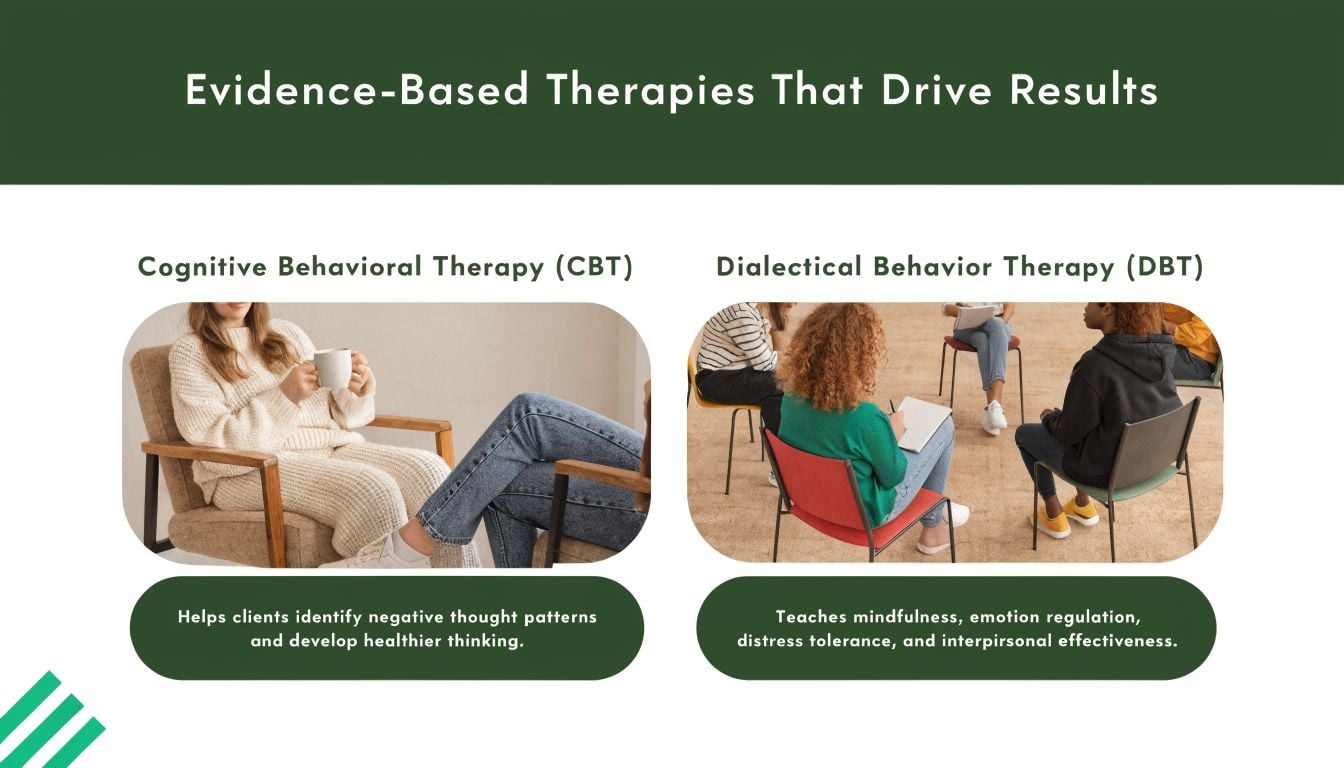
CBT and DBT for daily symptom control
Cognitive Behavioral Therapy, or CBT, helps patients identify the thought patterns that drive cravings, avoidance, shame, hopelessness, and self-defeating behavior. A person learns to catch the sequence early. The thought shifts, the emotional intensity drops, and the urge doesn’t automatically become action.
Dialectical Behavior Therapy, or DBT, is especially useful when a patient struggles with emotional flooding, impulsivity, self-harm urges, unstable relationships, or intense reactions to stress. DBT teaches distress tolerance, emotional regulation, and interpersonal skills that make sobriety more livable.
These aren’t abstract ideas. They solve concrete problems. The patient who drinks after every argument needs more than insight. That patient needs skills for surviving the hour after the argument without using.
EMDR, ERP, and trauma-focused work
Some symptoms won’t improve much until trauma or obsessive fear is treated directly.
- EMDR helps patients process traumatic memories that still trigger panic, avoidance, nightmares, or substance use.
- ERP is used when OCD symptoms are part of the picture. It helps patients face obsessive fears without performing the compulsive behavior that keeps the cycle alive.
- Motivational approaches help when a person is ambivalent, guarded, or afraid of what recovery will ask of them.
Good therapy in dual diagnosis care doesn’t chase every symptom at once. Clinicians prioritize what’s driving the most risk, then build outward.
Medication management and staffing matter
Medication can stabilize mood, reduce psychiatric symptom intensity, improve sleep, and support engagement in therapy. It isn’t a cure by itself, and it isn’t the answer for everyone. But in the right case, careful medication management gives the patient enough stability to benefit from the rest of treatment.
This level of integration requires specialized staffing. In a national U.S. study, only 18% of addiction programs and 9% of mental health programs achieved “dual diagnosis capable” status, according to the Dual Diagnosis Capability study. That finding tells families something important. A program can be well-intentioned and still not be built for co-occurring care.
For a practical overview of outcomes, families often find it useful to review whether dual diagnosis treatment is effective and then ask direct questions about staffing, psychiatric access, and trauma competence before admission.
Hallmarks of a High-Quality Treatment Program
Families often call after a frightening stretch at home. Substance use is getting worse, mental health symptoms are harder to predict, and every program on the screen claims to treat both. The key question is simpler. Which program is built to handle both problems at the same time, with enough structure to keep the patient safe and enough flexibility to treat the person, not just the diagnosis?
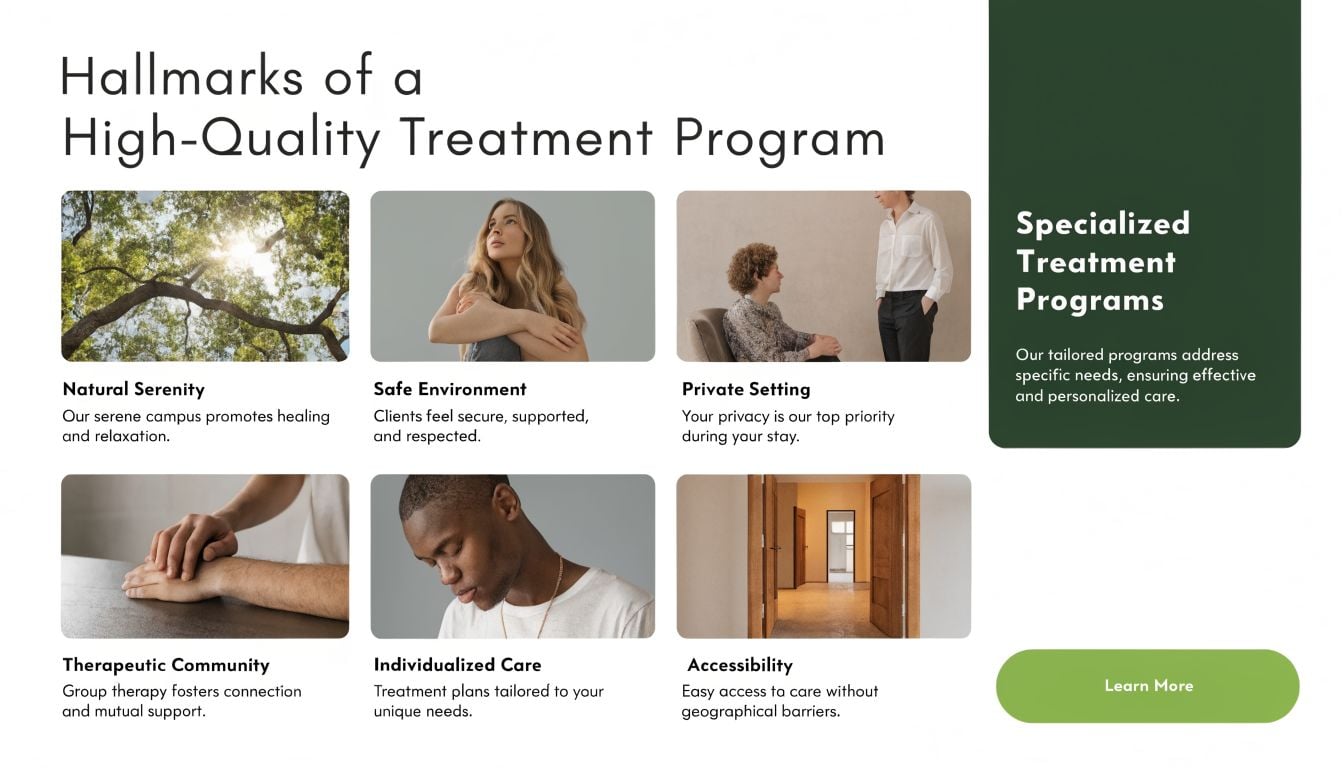
A strong program shows its quality in the details. Families should hear clear answers about who is providing care, how treatment plans are adjusted, what happens if symptoms change, and how discharge is handled long before the admission date arrives. Vague reassurance is not enough.
What to look for before saying yes
The best screening question is direct: how does this program treat co-occurring disorders in daily practice?
Look for these markers:
- Integrated assessment: the team reviews substance use, psychiatric symptoms, trauma history, medical needs, sleep, safety risk, and family stress as one clinical picture
- Licensed multidisciplinary staff: psychiatric providers, therapists, addiction clinicians, and nursing support all have a role when symptoms overlap
- Individualized treatment planning: care changes based on diagnosis, relapse history, motivation, and current level of functioning
- Family involvement: families get education, communication guidance, and a role in discharge planning when appropriate
- Step-down planning: the program prepares for the next level of care before the patient leaves
- Gender-specific programming when indicated: some patients engage more openly and make faster clinical progress in a setting designed for men or for women
In Massachusetts, this matters for practical reasons as much as clinical ones. Families are often trying to choose quickly, verify benefits, and avoid a failed placement. Reviewing how insurance coverage for addiction treatment usually works can help families ask better questions before they commit.
Why gender-responsive care deserves close attention
Gender-specific treatment is not a marketing feature. It can change what a patient is willing to say out loud, how safe group therapy feels, and how trauma work is paced.
In clinical practice, women with co-occurring disorders often need space to address trauma, caregiving strain, relationship patterns, body image concerns, and the effects of chronic stress without filtering themselves in a mixed setting. Men often benefit from a program that addresses shame, emotional restriction, anger, isolation, and accountability in a way that gets past defensiveness and into real work. These are patterns, not rules. The point is fit.
That is one reason gender-specific programming is a meaningful benchmark at Paramount Recovery Centers. It gives clinicians more room to tailor groups, improve participation, and address sensitive material without forcing every patient into the same format.
If a program uses the same structure for every patient, treatment gets easier for the program and less effective for the patient.
A high-quality provider should be able to explain, in plain language, how it handles trauma, medication oversight, family communication, relapse planning, and the different treatment needs that can show up across male and female populations. If the answers stay generic, keep asking questions. If your family is in crisis, the next right step is a call with an admissions team that can explain the model clearly and tell you whether the fit is right.
How to Navigate Admissions and Insurance in Massachusetts
A family usually calls at a hard moment. Someone has relapsed, stopped taking psychiatric medication, or agreed to treatment after weeks of conflict. That is not the time for a confusing intake process.
In Massachusetts, admissions should start with a clear phone assessment that helps you answer four questions quickly. Is the person safe right now? Do they need detox first? What level of care fits the combination of substance use and mental health symptoms? How soon can treatment begin?
At Paramount Recovery Centers, that first conversation is meant to turn panic into a plan. Families do not need every detail organized in advance. They need to describe what is happening now, list any medications if they can, and be honest about recent substance use, self-harm risk, psychosis, or prior treatment.
What admission usually includes
A well-run admissions process often follows this order:
- A clinical screening to assess safety, substance use, psychiatric symptoms, and immediate medical or detox needs.
- Insurance verification to clarify benefits, likely out-of-pocket costs, and any authorization requirements.
- Level-of-care planning to decide whether the patient should start with detox, residential care, or another setting.
- Admission coordination so the family knows what to bring, when to arrive, and what contact looks like after intake.
Speed matters here.
Dual diagnosis symptoms can shift fast. A person who asks for help in the morning may refuse it by evening. Another may look calmer once substances wear off, then become more depressed, paranoid, or medically unstable within a day. Programs that handle admissions well know how small that treatment window can be.
Insurance questions also stall families more than they should. The practical goal is not to master policy language. It is to confirm whether the plan covers behavioral health treatment in Massachusetts, whether preauthorization is required, and what services are included at the recommended level of care. Many families start by reviewing insurance coverage for addiction treatment so the first call is more productive.
Ask direct questions. Does the program treat mental health and substance use at the same time? Who manages psychiatric medications? Can the team place the patient in detox if needed? Is there gender-specific programming? How does family communication work during treatment?
Those answers tell you a lot about program quality.
One more practical point often gets missed. Early stabilization is not only about therapy and medication. Sleep disruption can intensify cravings, panic, irritability, and mood swings in the first phase of treatment, which is why families often benefit from learning about science-backed sleep habits as part of the larger recovery picture.
The next step is simple. Call while your loved one is still willing to talk, and let the admissions team help you decide what needs to happen first.
Begin Your Path to Lasting Recovery Today
Dual diagnosis can make a family feel trapped because the symptoms seem to contradict each other. A loved one may swear they need substances to cope, then become far more unstable because of them. They may want help and resist help in the same day. That confusion is common. It’s also treatable when care is built around both conditions at once.
Recovery usually becomes more stable when treatment addresses the whole picture. That includes psychiatric symptoms, substance use, sleep, trauma, relationships, medications, and the habits that shape daily life after discharge. Even simple routines matter. Families often benefit from learning about science-backed sleep habits because sleep disruption can intensify cravings, anxiety, and mood instability during early recovery.
The next step doesn’t have to be a lifelong commitment. It can just be a call. A real conversation with a trained admissions team can clarify whether detox is needed, what level of care fits, how insurance may apply, and how quickly treatment can start in Massachusetts.
Waiting rarely makes dual diagnosis simpler. Early action gives the patient a better chance to stabilize before another relapse, psychiatric emergency, or family rupture forces the issue.
If someone you love is struggling with both addiction and mental health symptoms, Paramount Recovery Centers can help you understand the next step and coordinate care. Call (888) 388-8660 for a confidential conversation about admissions, insurance, and dual diagnosis treatment options in Massachusetts.
