
Wanting to come off Suboxone often starts with two competing thoughts. One says it's time to move forward. The other says, “What if withdrawal hits, cravings come back, or everything unravels?”
That tension is normal. It also explains why a Suboxone taper program should never be treated like a self-directed experiment. A taper is a medical process that changes brain and body chemistry over time. When people try to rush it, skip monitoring, or cut doses based on how they feel on a single hard day, the plan usually becomes less safe and less effective.
A supervised taper does more than lower a prescription. It tracks stability, protects sleep, addresses anxiety, watches for relapse risk, and adjusts the pace when the body says the schedule is too aggressive. The end goal isn't just getting to zero. The goal is staying functional, protecting recovery, and building a plan for what comes next.
Starting Your Suboxone Taper Journey Safely

Many people reach this point after months or years of hard work. They've stabilized, rebuilt parts of life, and want to know whether tapering is possible. It may be possible. But “ready to ask about a taper” is not the same as “ready to stop quickly.”
The safest starting point is an honest clinical review. That review looks at current dose, time on Suboxone, recent opioid use history, psychiatric symptoms, stress at home, sleep, work demands, and whether cravings still break through under pressure. A taper should start only when those pieces are reasonably steady.
Why tapering alone creates avoidable risk
People who taper on their own tend to make predictable mistakes. They cut too much at once, confuse withdrawal with failure, and then either push harder or go back up chaotically. Neither pattern builds stability.
A medical team brings structure to the process:
- Assessment first: Clinicians confirm whether tapering is appropriate now, or whether maintenance remains the safer option.
- Planned reductions: Dose changes are scheduled instead of improvised.
- Symptom monitoring: Sleep disruption, anxiety, body aches, GI upset, and cravings are tracked in context.
- Course correction: If symptoms spike, the answer may be to hold, slow down, or step back briefly.
Going slower is not a setback. It's often what keeps a taper from turning into a relapse cycle.
What safe preparation looks like
Before the first dose reduction, patients need a few practical pieces in place.
- A prescriber-led plan with clear instructions.
- Behavioral support so stress, fear, and cravings don't drive dosing decisions.
- A relapse response plan for what to do if opioid thoughts intensify.
- Follow-up appointments close enough together to catch problems early.
In Massachusetts, a treatment setting that can coordinate medication management with therapy and step-up care offers the strongest safety net. That's what makes a structured program more than a taper calendar. It becomes a clinical partnership built to protect recovery.
What Is a Medically Guided Suboxone Taper
A medically guided taper is a structured reduction of buprenorphine/naloxone designed to let the body adjust gradually rather than all at once. The easiest way to think about it is as a dimmer switch, not a light switch. A controlled descent gives the nervous system time to adapt. Abrupt changes create unnecessary shock.
Suboxone doesn't just suppress withdrawal; it helps regulate cravings, lowers opioid reinforcement, and supports day-to-day stability. Taking it away too quickly can unsettle all three.
What the taper is actually trying to accomplish
A good taper aims for more than a lower dose on paper. It targets several goals at once:
- Reduce withdrawal burden: Symptoms may still appear, but the plan should keep them manageable.
- Protect daily function: Work, parenting, sleep, and relationships should remain as stable as possible.
- Monitor cravings closely: A patient who looks “fine” physically may still be at high relapse risk psychologically.
- Preserve judgment: Fear, irritability, and insomnia can push people toward impulsive decisions.
A taper that ignores any one of those areas is incomplete.
Why stability before tapering matters
Higher maintenance doses are associated with better treatment success. One research summary found that flexible dosing up to 32 mg/day was linked with a 20% greater success rate and a 20% lower risk of discontinuation, reinforcing the importance of starting from a stable, effective dose instead of rushing into dose reduction.
That principle shapes real clinical care. If someone is still cycling through cravings, unstable mood, or frequent missed doses, tapering usually adds pressure instead of solving the problem.
For readers who want a broader overview of how medication fits into recovery care, medication-assisted treatment basics can help clarify where a taper does and doesn't fit.
Clinical point: A taper should begin from stability, not from frustration with being on medication.
What medical oversight changes
Professional oversight affects decisions that seem small but matter a lot. Clinicians decide whether a symptom wave means “hold the dose,” “slow the taper,” or “look for another cause.” They also watch for the common trap of blaming every bad day on the taper when stress, depression, conflict, or poor sleep may be driving the crash.
A medically guided Suboxone taper also includes support beyond prescribing. Therapy, relapse prevention work, family involvement when appropriate, and practical planning all matter. That's why the medication endpoint isn't the whole treatment target. The primary target is durable recovery after the medication changes.
Understanding Suboxone Taper Schedules
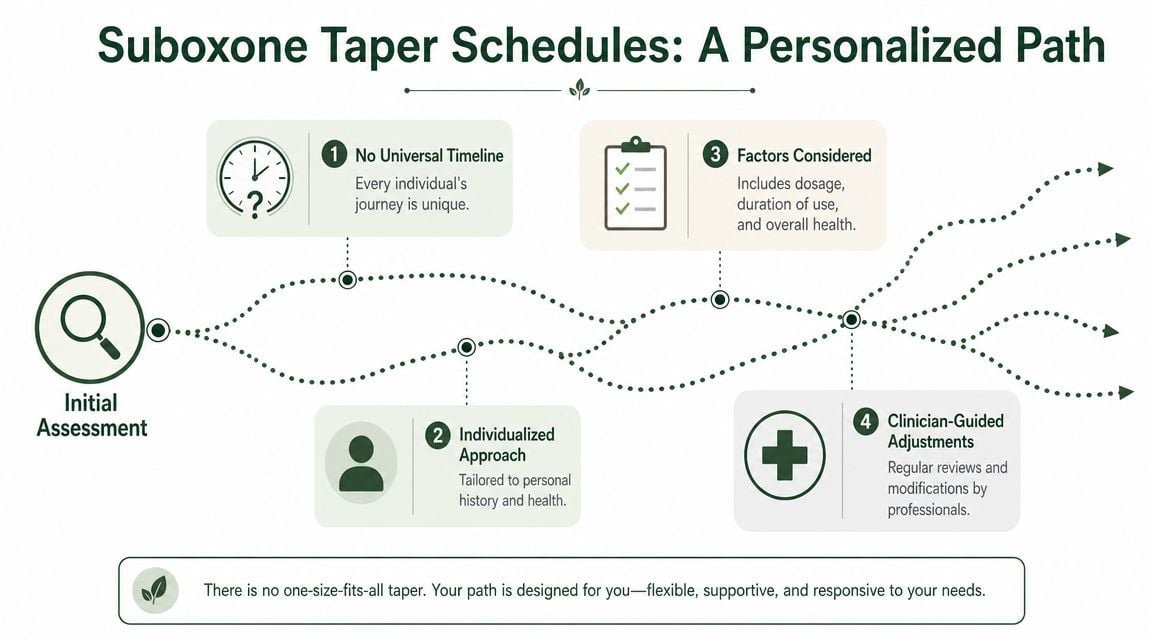
There is no universal taper schedule. Two patients can take the same starting dose and need very different pacing based on history, stability, co-occurring mental health symptoms, and what happens when reductions begin.
That's why a schedule should be built around response, not impatience. A calendar is useful. A rigid calendar is often a problem.
What clinicians look at before choosing a pace
A taper schedule starts with the patient in front of the clinician, not with a generic template. The most relevant factors usually include:
- Current effective dose: Higher or lower doses present different reduction challenges.
- Length of time on Suboxone: Longer treatment often calls for more patience.
- History of relapse: Repeated return to opioid use raises the need for caution.
- Mental health symptoms: Anxiety, depression, trauma symptoms, and insomnia can intensify as doses fall.
- Home and work stability: High conflict or unstable housing can make an outpatient taper harder to sustain.
The role of gradual dose reductions
Practical taper guidance commonly recommends reducing dose by no more than 25% every 1 to 2 weeks, with slower reductions at lower doses, because smaller decrements are often better tolerated and clinicians may need to pause or briefly increase the dose if symptoms intensify (practical taper guidance for Suboxone dose reduction).
That isn't a rule to force on every patient. It's a reminder that the body often tolerates controlled, measured changes better than aggressive cuts. The closer the dose gets to the low end, the more important those small adjustments become.
Faster and slower tapers are not a simple good-bad choice
Some readers assume a longer taper must always produce better outcomes. The evidence doesn't support that assumption by itself. In a multi-site trial of 516 participants, the 7-day taper group had 44.3% opioid-negative urine tests at the end of taper compared with 29.9% in the 28-day group, with P=0.0007. But that short-term advantage disappeared at follow-up. Rates were 18% vs. 18% at 1 month and 12% vs. 13% at 3 months for the 7-day and 28-day groups, respectively (multi-site buprenorphine taper trial findings).
The lesson isn't that fast tapers are better. The lesson is that taper speed alone doesn't determine long-term success.
A schedule can get someone through detox. It cannot replace aftercare, relapse prevention, and clinical follow-up.
What a workable schedule usually includes
Rather than focusing on how quickly the number reaches zero, clinicians usually want a schedule that includes:
| Clinical focus | Why it matters |
|---|---|
| Starting from a stable dose | Reduces the chance that tapering begins during an unstable period |
| Planned check-ins | Catches sleep disruption, cravings, and mood changes early |
| Flexible holds | Gives the body time to catch up after difficult reductions |
| Behavioral support | Helps the patient manage triggers that medication had been buffering |
A strong taper schedule is personal, adjustable, and tied to recovery goals outside the prescription bottle.
Managing Withdrawal Symptoms and Cravings
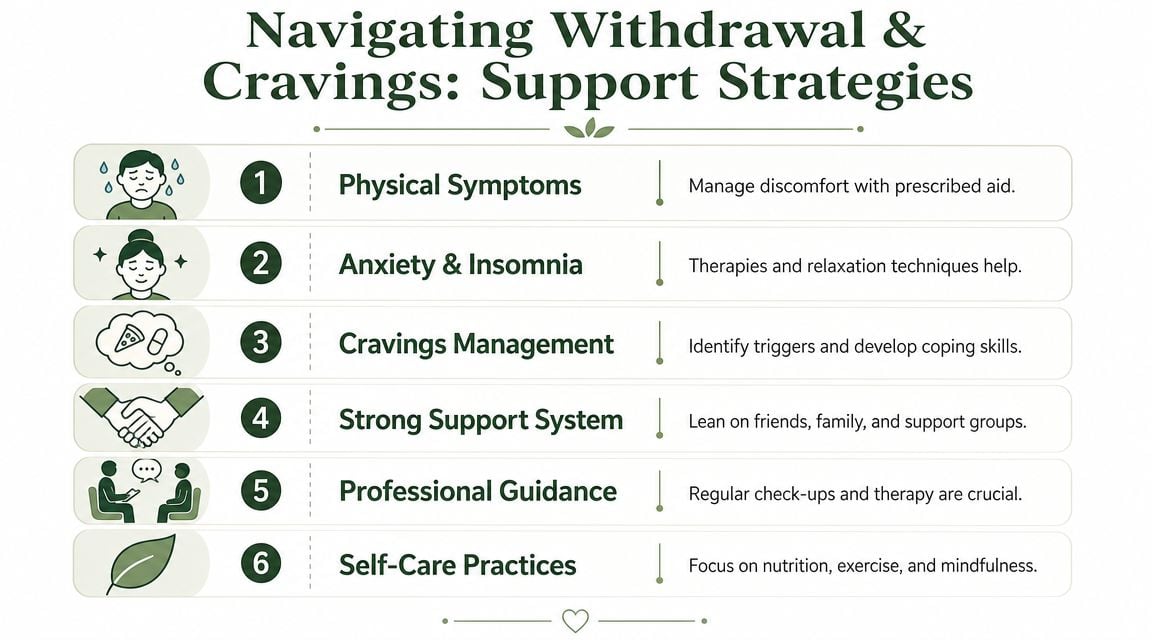
Withdrawal is the part many individuals fear before a Suboxone taper starts. That fear is reasonable. Symptoms can include anxiety, restlessness, insomnia, irritability, body aches, chills, sweating, GI upset, low mood, and increased sensitivity to stress.
The key point is that discomfort does not automatically mean the taper is failing. It often means the body has noticed the change and needs the plan adjusted.
What clinicians do when symptoms rise
Medical supervision changes the response to symptoms. Instead of guessing, the team looks at timing, severity, function, and relapse risk. Then they decide whether to hold the dose, slow the next reduction, or add non-addictive symptom support.
Common supports during a taper may include:
- Sleep strategies: Structured sleep hygiene, schedule consistency, and treatment planning around insomnia.
- Anxiety management: Therapy, breathing work, grounding skills, and closer follow-up.
- Craving response plans: Trigger mapping, emergency contacts, and same-day clinical communication when risk rises.
- Lifestyle supports: Hydration, routine meals, movement, and predictable daily structure.
Why the final stretch often feels harder
Many patients find that tapering becomes more difficult below about 2 mg/day, when withdrawal symptoms can become more pronounced and expert guidance often requires slowing the pace or using smaller decrements.
Many self-directed tapers frequently fall apart. A patient may do reasonably well through the middle of the process, hit the low-dose range, and then assume they should push through the hardest part quickly. Clinically, that's usually the wrong move.
Practical rule: The last part of the taper often needs the most patience, not the least.
Cravings are not only physical
Cravings during a taper don't always show up as a direct urge to use opioids. Sometimes they appear as agitation, bargaining, obsession with dose timing, or the belief that one external stressor is “too much” without relief. That's why therapy has to run alongside medication changes.
For patients whose taper is stirring up panic, racing thoughts, or chronic worry, resources on counseling approaches can be useful. Some readers may benefit from reviewing Interactive Counselling for anxiety to better understand how targeted anxiety treatment supports recovery work.
What helps patients stay steady
A successful symptom-management plan usually includes both structure and flexibility.
- Keep the schedule visible: Patients do better when they know what change is coming next.
- Report symptoms early: Waiting until distress is severe makes rescue harder.
- Don't chase relief with impulsive changes: Taking more or less medication without guidance destabilizes the plan.
- Use support on ordinary days: Therapy and coping skills work best before a crisis peaks.
The goal isn't a symptom-free taper. The goal is a safe, tolerable process that doesn't push the patient back toward opioid use.
Choosing Your Path Inpatient vs Outpatient Tapers
The right taper setting depends on risk, structure needs, psychiatric symptoms, and the stability of the home environment. Some patients can taper while living at home and keeping a routine. Others need a more protected setting because too many triggers sit just outside the front door.
Neither option is automatically better. The better option is the one that matches the patient's real-world risk.
Inpatient vs Outpatient Suboxone Taper Comparison
| Feature | Inpatient Taper Program | Outpatient Taper Program |
|---|---|---|
| Supervision | Close daily monitoring in a structured environment | Regular appointments with monitoring between visits |
| Environment | Removed from many outside triggers and daily pressures | Patient remains in normal home, work, and family settings |
| Best fit | Higher relapse risk, unstable home life, active psychiatric symptoms, poor self-management | Strong support system, stable housing, reliable follow-through, manageable symptom burden |
| Schedule | Highly structured treatment day | More flexibility around work and family duties |
| Therapy access | Integrated throughout the day | Scheduled sessions during the week |
| Response to setbacks | Rapid escalation of support available on site | Requires prompt communication and possible step-up in care |
When inpatient care makes more sense
An inpatient taper is often the better fit when someone has repeated relapse history, high anxiety, severe insomnia, dual-diagnosis concerns, or a home situation that makes recovery hard to protect. It also helps when the person wants to taper but can't reliably follow a plan outside a structured setting.
When outpatient can work well
Outpatient tapering can work when the patient is medically and psychiatrically stable, has transportation, shows consistent follow-through, and has people around them who support recovery instead of undermining it. Some patients do best because they can continue parenting or work responsibilities while still receiving treatment.
For readers weighing these models in more detail, it can help to compare outpatient recovery programs and also review this guide to inpatient vs outpatient rehab options.
The setting should match the level of support needed to finish the taper and stay safe after it ends.
The Paramount Recovery Centers Approach
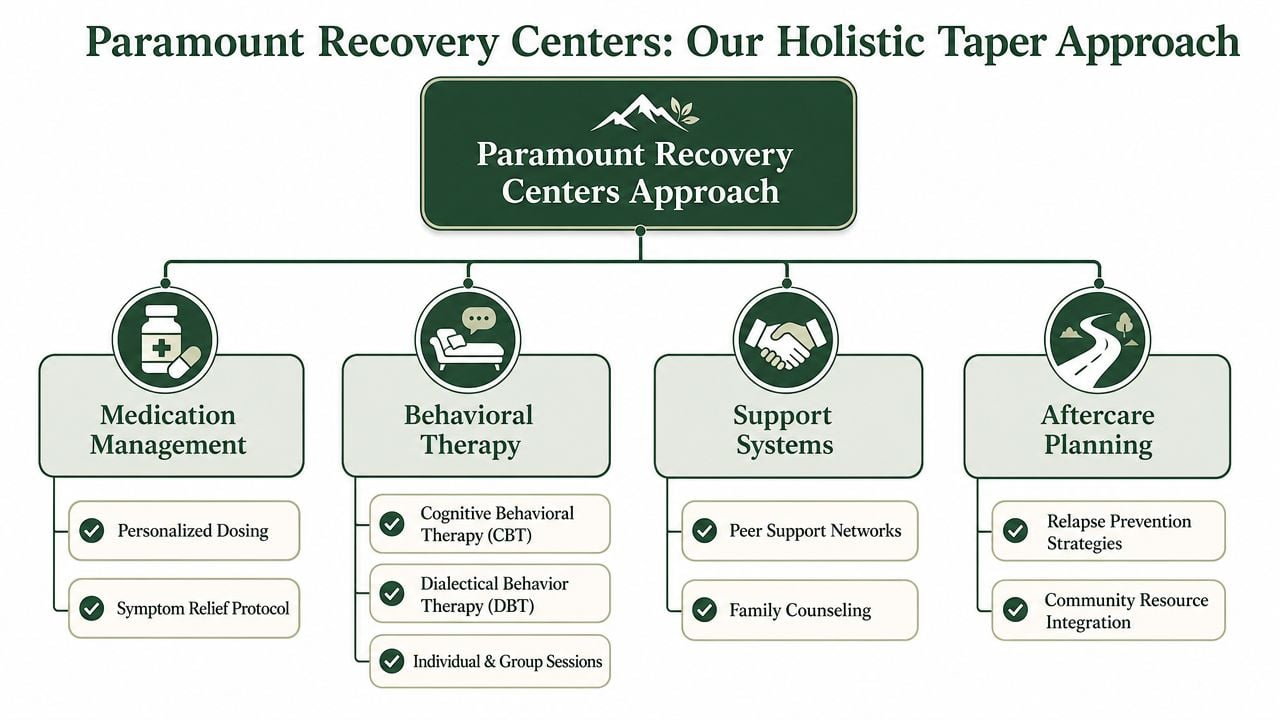
A Suboxone taper works best when it sits inside a larger treatment plan. Medication management matters, but it can't carry the whole process by itself. The stronger model combines taper planning with therapy, relapse prevention, mental health care, family work, and aftercare preparation.
Whole-person care during a taper
At Paramount Recovery Centers, a taper can be coordinated with a broader continuum of care that includes medication management, individual therapy, group therapy, dual-diagnosis treatment, and step-up or step-down support when needed. That matters because many taper setbacks are driven less by the dose itself and more by untreated anxiety, trauma symptoms, depression, family conflict, or unstable routines.
A whole-person model addresses those drivers directly.
- Medication management: Dose adjustments are tied to symptom response and stability.
- Therapy integration: Patients build coping tools while the medication buffer is gradually reduced.
- Family involvement: Loved ones learn how to support the process without policing it.
- Aftercare planning: The work after the final dose is prepared before the taper ends.
Why dual-diagnosis treatment matters
A patient with untreated panic symptoms may call the taper “impossible” when the underlying issue is rising anxiety. A patient with trauma triggers may interpret normal stress as a sign they need immediate relief. A patient with depression may lose motivation and stop attending appointments.
Those are treatment issues, not character flaws. When mental health care runs alongside the taper, clinicians can tell the difference between withdrawal, relapse risk, and a co-occurring psychiatric condition that needs direct attention.
Recovery skills must outlast the taper
A taper is a transition, not a graduation ceremony. The medication decreases while recovery responsibilities increase. Patients need tools for cravings, conflict, boredom, poor sleep, shame, social pressure, and the ordinary stress of life without relying on rapid symptom relief.
That's why the most effective programs don't end the moment the Suboxone dose ends. They continue with relapse prevention planning, ongoing therapy, community support, and follow-up. The medication may change. The treatment relationship shouldn't disappear at the point it becomes most important.
Your Next Steps and Common Questions
A safe Suboxone taper depends on partnership. The medication is reduced gradually, symptoms are monitored, mental health is treated alongside substance use, and aftercare is planned before the taper is over. That's what protects recovery.
People who do best usually stop asking, “How fast can this be over?” and start asking, “What support do I need to do this safely?”
Common questions patients ask
Does insurance cover a Suboxone taper program
Coverage depends on the plan, the level of care, medical necessity, and whether therapy, medication management, or a higher-support setting is recommended. The fastest way to get a clear answer is to verify benefits directly with admissions staff before treatment begins.
How does someone start the admissions process
The process usually begins with a confidential call, a clinical screening, insurance verification, and a recommendation for the appropriate level of care. Patients who want to understand how qualified prescribing and treatment oversight work can review this guide to a Suboxone doctor and addiction treatment specialist.
What happens after the taper is complete
The end of Suboxone should lead into continued recovery care, not a treatment vacuum. That may include therapy, relapse prevention work, alumni support, psychiatric follow-up, family sessions, and monitoring during the period when cravings or mood changes could still reappear.
What if anxiety gets worse during the taper
That's common enough that it should be anticipated, not hidden. A taper plan should include mental health support, coping tools, and a clear protocol for reassessment if anxiety starts to interfere with sleep, function, or safety. For a broader mental health perspective, some readers may find The Lagom Clinic's therapy insights useful alongside addiction-specific care.
The next right step is simple. Call a treatment team, get evaluated honestly, and let the taper be built around medical reality instead of fear or pressure. For immediate help, compassionate admissions support is available 24/7 at (888) 388-8660.
A CTA for Paramount Recovery Centers. If Suboxone has helped create stability, the next phase deserves the same level of care. Call (888) 388-8660 to speak with admissions about a medically supervised taper, treatment options in Massachusetts, insurance verification, and the support needed before, during, and after the taper.
