

A lot of families in Massachusetts reach this point in silence. A husband says he’s just under stress. A father promises he can stop after this week. A brother keeps going to work, paying bills, and acting normal while alcohol, opioids, cocaine, or pills start running more of his life than anyone wants to admit.
Men often hold the line longer than people realize. They hide symptoms, minimize consequences, and tell themselves they should be able to handle it alone. That silence can look like strength from the outside. In practice, it often means addiction gets more time to grow.
That’s why men's substance abuse treatment matters. Recovery for men isn’t only about removing a substance. It’s about treating the pressure, shame, isolation, and habits that often keep men stuck. When care matches how men tend to enter treatment, communicate distress, and respond to structure, treatment becomes more than a crisis response. It becomes a real path forward.
The First Step Can Be the Hardest
A man may know something is wrong long before he asks for help. He may be drinking after work every night, using drugs to get through stress, or moving between brief attempts to stop and painful returns to use. His family may see the mood swings, missed commitments, and growing tension at home. Still, many men wait.
They wait because asking for help can feel like surrender. It can feel like admitting failure as a provider, partner, or parent. For some men, the deeper fear isn’t treatment itself. It’s the idea of sitting in a room and saying out loud what they’ve spent years trying not to feel.
What families usually notice first
Families often don’t see addiction as one dramatic event. They see a pattern.
- Shorter tempers: Small frustrations turn into arguments or withdrawal.
- Changing routines: Sleep, eating, work habits, and social behavior start shifting.
- Broken promises: A man means what he says in the moment, then can’t follow through.
- Emotional distance: He may still be present physically, but he’s harder to reach.
Those signs matter because addiction rarely stays contained. It affects work, health, relationships, finances, and self-respect.
Treatment works better when the first call happens before everything falls apart.
Why hesitation is so common
Men are often taught to solve problems privately. That mindset can help at work or in a crisis. It doesn’t help when substance use has become the coping system itself.
A strong treatment process meets that reality without judgment. It explains what happens next, makes admissions simple, and gives men a clear structure instead of vague advice to “just get help.” That clarity lowers fear. It also helps families stop guessing and start acting.
Why Men's Addiction Treatment Is Different
Men don’t need softer messaging. They need treatment that fits the way many of them experience distress, defend against it, and finally enter care. Gender-responsive treatment isn’t a branding idea. It addresses real clinical barriers that show up again and again.

Men also show a disproportionate need for treatment. In 2020, 64.9% of publicly funded drug rehabilitation admissions were male, even though men made up about 49% of the population, according to data on addiction in men. That gap points to more than prevalence alone. It also reflects the way men delay care, escalate risk, and often arrive in treatment after the problem has become harder to manage.
Stoicism changes how men ask for help
Many men don’t describe depression, fear, grief, or trauma in direct language. They describe pressure. Irritability. Trouble sleeping. Anger. Numbness. Needing to shut off their mind.
That matters in treatment. A program that expects quick emotional openness from day one may lose men who are still testing whether it’s safe to be honest. Good men's substance abuse treatment uses direct conversation, practical goals, and a structure that helps men build trust before they’re asked to do deeper emotional work.
A helpful outside perspective appears in Ben's article on gender in therapy, which discusses how gender can shape communication and engagement in counseling. That idea matters in addiction care, where the wrong therapeutic style can feel mismatched before treatment has a chance to work.
Men often respond better to action-oriented care
Some men engage more fully when therapy feels concrete. They want to know what the trigger was, what the pattern is, and what to do differently the next time. That doesn’t mean they’re avoiding emotion. It means they often reach emotion through structure.
Programs built for men usually work better when they include:
- Clear goals: Specific treatment targets are easier to commit to than abstract self-exploration.
- Practical skill building: Men often stay engaged when they can apply what they learn immediately.
- Direct accountability: Honest feedback, done well, reduces denial without creating shame.
- Peer identification: Men often open up faster when they hear their own struggles reflected by other men.
Some men won’t begin with “I’m hurting.” They’ll begin with “I’m tired of living like this.” That’s enough to start.
What doesn’t work well
A one-size-fits-all model often misses the reasons men use in the first place. It may focus on stopping behavior without understanding the identity threat underneath it. If a man believes treatment will strip him of control, expose him, or judge him, he’s more likely to leave early or hold back.
The better approach gives him a place to be honest without performing toughness, and without being reduced to it.
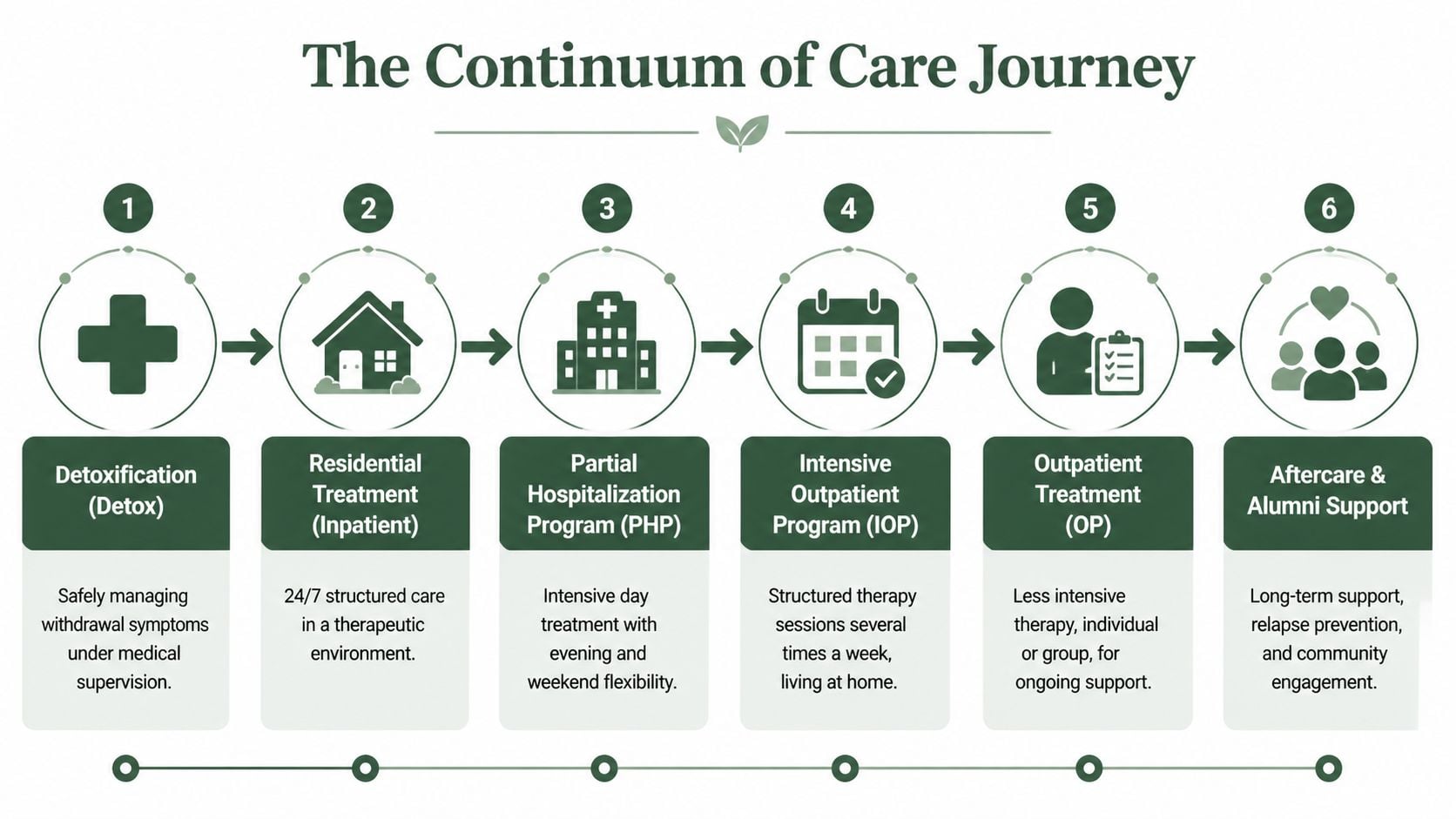
Understanding the Full Continuum of Care
Individuals don’t need one generic level of treatment. They need the right level at the right time, and they often need to move through several stages. That’s what a continuum of care means. It creates a recovery path instead of a single treatment event.
National admissions data shows why flexibility matters. According to 2022 TEDS data, the most common levels of care for admissions are non-intensive outpatient at 41.5%, residential detox at 13.3%, and intensive outpatient at 11.2%, as reported in the 2022 treatment admissions summary. People enter care at different levels because severity, home stability, withdrawal risk, work demands, and mental health all differ.
What each level of care is for
A full system should let treatment intensity rise or step down based on need.
| Level of Care | Environment | Time Commitment | Best For |
|---|---|---|---|
| Detox placement | Medically supervised setting | Short-term, based on withdrawal needs | Men who may need clinical support to stop safely |
| Residential treatment | Live-in therapeutic setting | Full-day, immersive care | Men who need distance from triggers and round-the-clock structure |
| PHP | Day treatment with return home or sober housing at night | Most of the day, several days a week | Men who need strong support without overnight stay |
| IOP | Outpatient clinical setting | Several sessions each week | Men transitioning from higher care or needing more flexibility |
| OP | Standard outpatient setting | Lower weekly commitment | Men with stable functioning who still need therapy and accountability |
| Aftercare and alumni support | Community-based ongoing support | Long-term, individualized | Men protecting recovery after formal treatment |
How the progression usually works
A useful way to think about care is to think in layers.
- Safety first. Detox placement handles withdrawal risk and immediate stabilization.
- Structure next. Residential or PHP creates distance from chaos and builds a daily recovery rhythm.
- Re-entry planning. IOP and outpatient care help a man practice recovery while dealing with real-life stressors again.
- Long-term support. Aftercare keeps treatment gains from fading once the crisis has passed.
For families unsure how much care is enough, guidance on a full continuum of care for addiction recovery can help clarify what step-down planning looks like.
A man doesn’t fail treatment because he needs more than one level of care. That often means treatment is being matched to reality.
The real trade-off
Lower levels of care preserve more daily freedom. Higher levels provide more containment and support. Neither is automatically better. The right choice depends on safety, relapse history, mental health, home environment, and whether the man can follow through outside a structured setting.
That decision should be clinical, not emotional. Families often want the least disruptive option. Addiction often responds better to the most appropriate option.
Evidence-Based Therapies Proven to Work for Men
The setting matters, but the therapy itself is what changes behavior. Men’s treatment works best when therapy isn’t just offered, but matched to how men tend to defend, rationalize, avoid, and recover.

Structured therapies can be especially effective. Effective approaches such as CBT and Relapse Prevention Training can yield 20 to 30% higher retention rates in men compared with mixed-gender groups, according to the UK adult substance misuse treatment report. Retention matters because men often enter treatment ambivalent, guarded, or skeptical. The longer they stay engaged, the more likely deeper change becomes possible.
CBT helps men interrupt the pattern
Cognitive Behavioral Therapy works well for many men because it makes addiction visible. It identifies the sequence. Trigger, thought, urge, action, consequence. That structure reduces shame because it turns a vague sense of failure into a pattern that can be changed.
CBT can help a man recognize beliefs such as:
- “I need something to calm down.”
- “I’ve already messed up today, so it doesn’t matter.”
- “No one can help me anyway.”
When those thoughts are challenged and replaced, behavior starts to move.
Relapse prevention gives men a plan they can use
Relapse prevention is practical by design. It teaches men to identify high-risk situations, rehearse responses, and prepare for the times they’re most likely to justify using.
That may include a Friday night after work, an argument with a partner, isolation in a hotel room, or a spike in shame after making a mistake. Good relapse prevention doesn’t rely on motivation alone. It uses routines, accountability, and preplanned decisions.
Clinical reality: Motivation rises and falls. A recovery plan has to keep working on the days a man doesn’t feel inspired.
Trauma work matters even when a man never calls it trauma
Many men don’t arrive saying they need trauma treatment. They may talk about violence, loss, humiliation, accidents, neglect, military experiences, childhood instability, or constant hypervigilance without ever using that word.
That’s where trauma-focused methods such as EMDR can help. They address the unresolved material that keeps fueling substance use, panic, anger, numbness, or compulsive escape.
Family therapy also plays a major role. It helps repair trust, reduce enabling, and address the rigid roles that often form around addiction. In many homes, one person overfunctions while the man using substances underfunctions. Treatment should correct that system, not just the substance use.
For families comparing treatment methods, this overview of the best forms of therapy for addiction recovery offers a useful starting point.
Treating Addiction and Co-Occurring Disorders Together
A man can stop drinking or using drugs for a short period and still remain at high risk if the mental health side is untouched. That’s one of the most common reasons treatment falls short. The substance may be removed, but the emotional engine driving it is still running.
This is especially important in men's substance abuse treatment because men often self-medicate symptoms they haven’t named. They may call it stress, anger, burnout, or not sleeping. Underneath that, there may be depression, anxiety, trauma, grief, or panic.
Why separate treatment fails
When mental health and addiction are treated as separate issues, each one can reactivate the other. Depression drains motivation. Anxiety increases cravings for relief. Trauma symptoms make numbing feel urgent. Then relapse creates more shame, which worsens the mental health symptoms again.
The relationship is well established. Co-occurring depression is found in up to 40% of male SUD cases, and effective treatment has to address both conditions at the same time to reduce relapse risk, as noted qualitatively from the earlier treatment data source.
What integrated care actually looks like
Integrated treatment means one coordinated plan, not two disconnected tracks. It usually includes:
- Psychiatric evaluation: To identify depression, anxiety, trauma symptoms, mood instability, or other concerns early.
- Therapy that addresses both sides: A therapist should understand how mental health symptoms and substance use trigger each other.
- Medication management when appropriate: Medication can support stabilization, but it should be part of a broader plan.
- Skills for daily functioning: Men need practical tools for sleep, conflict, emotional regulation, and stress tolerance.
A man who drinks to quiet panic won’t stay stable for long if treatment only tells him to stop drinking.
What families should look for
Families should ask whether the program treats dual diagnosis in the same setting, with coordinated clinical oversight. If the answer is vague, treatment may become fragmented.
A strong program should be able to explain how therapy, medication support, recovery planning, and family involvement work together. That integrated model gives men a better chance at lasting recovery because it treats the cause and the coping method at the same time.
How to Choose a Men's Treatment Program in Massachusetts
Choosing a program can feel overwhelming when everything is urgent. Families often compare websites, call multiple centers, and still come away unsure what matters. The goal isn’t to find the most polished language. It’s to find a program that can safely assess, admit, and treat the problem in front of them.

Access matters because too many people never make it into care. In 2024, 52.6 million people needed SUD treatment, but only 23% received it, according to national addiction treatment statistics and demographics. A complicated intake process, slow callbacks, or unclear placement recommendations can cost valuable time.
A practical checklist for Massachusetts families
When evaluating men's substance abuse treatment, these questions help separate strong programs from weak ones.
- Does the program offer more than one level of care: Men often need movement between structured treatment stages, not a single fixed service.
- Is dual-diagnosis treatment built in: A program should be ready to treat mental health conditions alongside substance use.
- Are therapies evidence-based: Look for approaches such as CBT, trauma-focused care, relapse prevention, family work, and medication support when appropriate.
- Is the admissions process responsive: Fast insurance verification and clear next steps reduce dropout before treatment starts.
- Does the environment fit men’s needs: A men-focused track should understand shame, avoidance, identity pressure, and the need for direct accountability.
What to ask on the first phone call
The first call should produce clarity, not confusion. Families should ask:
- What level of care fits his current situation
- How quickly can the team complete an assessment
- What happens if detox is needed first
- How is mental health evaluated
- What support is offered after primary treatment
If a program can’t answer those questions clearly, the process may become fragmented later.
For readers weighing options locally, this guide to choosing a rehab facility in Massachusetts covers the practical details families should review before making a decision.
One Massachusetts option to consider
Paramount Recovery Centers is a Southborough-based addiction and mental health treatment provider that offers detox placement, inpatient treatment, PHP, intensive and standard outpatient care, dual-diagnosis support, family therapy, and aftercare for adults across Massachusetts. For men who need a gender-responsive track and a coordinated path through different levels of care, that kind of full-service model can reduce delays and treatment gaps.
Your Path to Recovery Starts with One Call
Men often wait for a bigger consequence before accepting help. Another missed commitment. Another scare. Another family crisis. That delay usually makes treatment harder, not easier.
The better move is to act when the problem is clear enough to name. A man doesn’t need to lose everything to qualify for real help. He needs an assessment, a plan, and a treatment team that understands why men often stay silent until they’re exhausted.
What that call can do
A confidential admissions call can help answer the questions families usually carry alone:
- Does he need detox first
- What level of care makes sense right now
- How quickly can treatment begin
- Will insurance help cover care
- What should the family do next
Those questions don’t need to be sorted out in isolation. Waiting tends to protect the addiction. Action protects the person.
“You don’t need perfect certainty before reaching out. You only need enough honesty to say that what’s happening isn’t working.”
If a man in Massachusetts is struggling, or if his family is running out of ways to help, the next step is simple. Call (888) 388-8660. The conversation can be confidential, direct, and focused on what comes next. That one call can turn panic into a plan.
If help is needed now, Paramount Recovery Centers offers confidential admissions support for adults in Massachusetts seeking addiction and mental health treatment. Call (888) 388-8660 to discuss treatment options, insurance verification, and the next appropriate level of care.
