

Stopping Zoloft can stir up a very specific kind of fear. A person may be relieved to come off the medication, unsure whether it’s still needed, or worried that side effects and long-term use have become their own burden. At the same time, that person may be asking the same urgent question most families ask first: how long does Zoloft withdrawal last?
The short answer is that there isn’t one timeline for everyone. For many people, symptoms begin within days, often feel worst early on, and then gradually improve. For others, especially after long-term use or a fast taper, the process can last much longer and feel more disruptive than they expected.
That uncertainty is often what makes withdrawal so stressful. People don’t just feel dizzy, nauseated, emotionally raw, or unable to sleep. They also wonder whether what they’re feeling is normal, dangerous, or a sign that their original depression or anxiety is coming back. Families often don’t know what to watch for either.
A clear plan matters. So does good clinical judgment, especially when alcohol use, drug use, trauma, OCD, or another mental health condition is also part of the picture. In Massachusetts, many people aren’t just managing Zoloft withdrawal. They’re managing Zoloft withdrawal while also trying to stay sober, stabilize mood, repair sleep, and keep daily life from falling apart.
Navigating Your Journey Off Zoloft Safely
The safest way to think about Zoloft withdrawal is this: it’s a transition, not a test of willpower.

When someone reduces or stops sertraline, the body and brain need time to adjust. Clinicians call the reaction antidepressant discontinuation syndrome. That term sounds technical, but the experience is familiar to many patients: dizziness, nausea, brain zaps, anxiety, sleep disruption, fatigue, and a flu-like sense that something feels off.
Withdrawal doesn’t mean someone has done anything wrong. It also doesn’t mean the medication was harmful. It means the nervous system adapted to a steady medication level and now has to function without it.
What concerned individuals and families should know first
A few practical rules make this process safer from the start:
- Don’t stop suddenly without guidance. Fast reductions tend to hit harder and create more confusion.
- Track timing carefully. Symptoms that begin soon after a dose change often fit withdrawal more than relapse.
- Watch function, not just discomfort. Missing work, isolating, drinking more, or becoming unable to sleep are meaningful warning signs.
- Take dual diagnosis seriously. If someone also struggles with alcohol, cannabis, stimulants, opioids, or sedatives, the withdrawal picture gets more complicated.
Practical rule: The more moving parts a person has, mood symptoms, substance use, trauma, sleep disruption, or past withdrawal difficulty, the less wise it is to manage Zoloft withdrawal casually.
A careful taper usually works better than a rushed one. Support works better than guessing. Families also do better when they stop debating whether symptoms are “real” and focus instead on what’s happening in front of them.
The goal isn’t just getting off the medication
The goal is preserving stability while the medication changes.
That means protecting sleep, preventing relapse into substance use, keeping anxiety from spiraling, and recognizing when outpatient support is enough and when a higher level of care is the safer move. For some people, the process is uncomfortable but manageable. For others, especially those with co-occurring substance use, it needs structured clinical oversight.
Why Zoloft Withdrawal Happens in the First Place
A common call to our team sounds like this: someone lowered Zoloft, then a few days later they felt dizzy, anxious, emotionally raw, and unsure whether they were getting sick, relapsing, or reacting to the medication change. If alcohol, cannabis, stimulants, or sedatives are also in the picture, that confusion grows fast. The timeline gets harder to read, and the safest response usually becomes slower, more structured, and more clinically supervised.
The brain adapts to regular sertraline exposure
Zoloft, or sertraline, is an SSRI. It changes serotonin signaling over time, and the brain adjusts to that steady input. Once the dose drops or the medication stops, the nervous system has to re-balance.
That process is the core reason withdrawal happens.
This does not mean Zoloft causes addiction in the same sense as alcohol, opioids, or benzodiazepines. It means the brain has adapted to a medication being present every day, and readjustment can be uncomfortable when that pattern changes too quickly. During that readjustment, people can develop a mix of physical, emotional, and cognitive symptoms, including dizziness, nausea, irritability, sleep disruption, poor concentration, and the sensory shifts many people describe as “brain zaps.”
For readers comparing withdrawal symptoms across medications, this overview of depression medication side effects helps explain why medication changes can affect both mood and the body at the same time.
Why symptoms can show up soon after a dose change
Sertraline does not stay in the body very long compared with some other psychiatric medications. As the level falls, the gap between what the brain has adjusted to and what it is now receiving becomes more noticeable. That is why symptoms often begin soon after a reduction, especially if the taper was rushed, doses were skipped, or the medication was stopped abruptly.
In practice, families often expect withdrawal to start only after the drug is fully out of the body. That is not how it usually works. The harder part is often the brain’s adjustment after blood levels begin to fall, not the exact moment the medication clears.
Dual diagnosis changes the picture
Generic advice often fails people in this context.
If someone also uses alcohol to sleep, cannabis to calm down, stimulants to get through the day, or benzodiazepines to manage panic, Zoloft withdrawal rarely happens in isolation. Each substance can affect sleep, anxiety, appetite, heart rate, mood stability, and sensory sensitivity. The result is a more complicated clinical picture where one set of symptoms can mask another.
For example, alcohol can temporarily blunt distress and then worsen insomnia, anxiety, and low mood as it wears off. Cannabis may reduce tension for a few hours while increasing derealization, panic, or rebound anxiety in others. Sedatives can cloud whether dizziness or agitation comes from SSRI withdrawal, sedative dependence, or both. This is one reason a dual-diagnosis assessment matters. The treatment plan has to account for all the active variables, not just the antidepressant.
People who want a broader overview of common withdrawal symptoms across substances and medications often find it easier to understand why co-occurring substance use can stretch out recovery and make symptom tracking less straightforward.
Withdrawal and relapse are not the same problem
Clinically, one of the most important questions is whether symptoms reflect antidepressant withdrawal, a return of depression or anxiety, substance-related effects, or some combination of the three.
Withdrawal usually tracks more closely to a dose reduction and often includes physical or neurological symptoms that stand out. Relapse tends to build more gradually and may look more like the original condition. In dual-diagnosis cases, the distinction matters even more because treating the wrong problem can make the person feel worse. Increasing structure, slowing the taper, addressing substance use, or shifting to a higher level of care may be safer than assuming the medication “stopped working.”
The primary goal is not just to get through a few hard days. It is to reduce suffering without destabilizing mood, sleep, or sobriety.
The Typical Zoloft Withdrawal Timeline and Symptoms
Individuals asking how long Zoloft withdrawal lasts typically seek a calendar. That’s understandable. They want to know when it starts, when it peaks, and when they can expect relief.
This visual gives a simple overview.
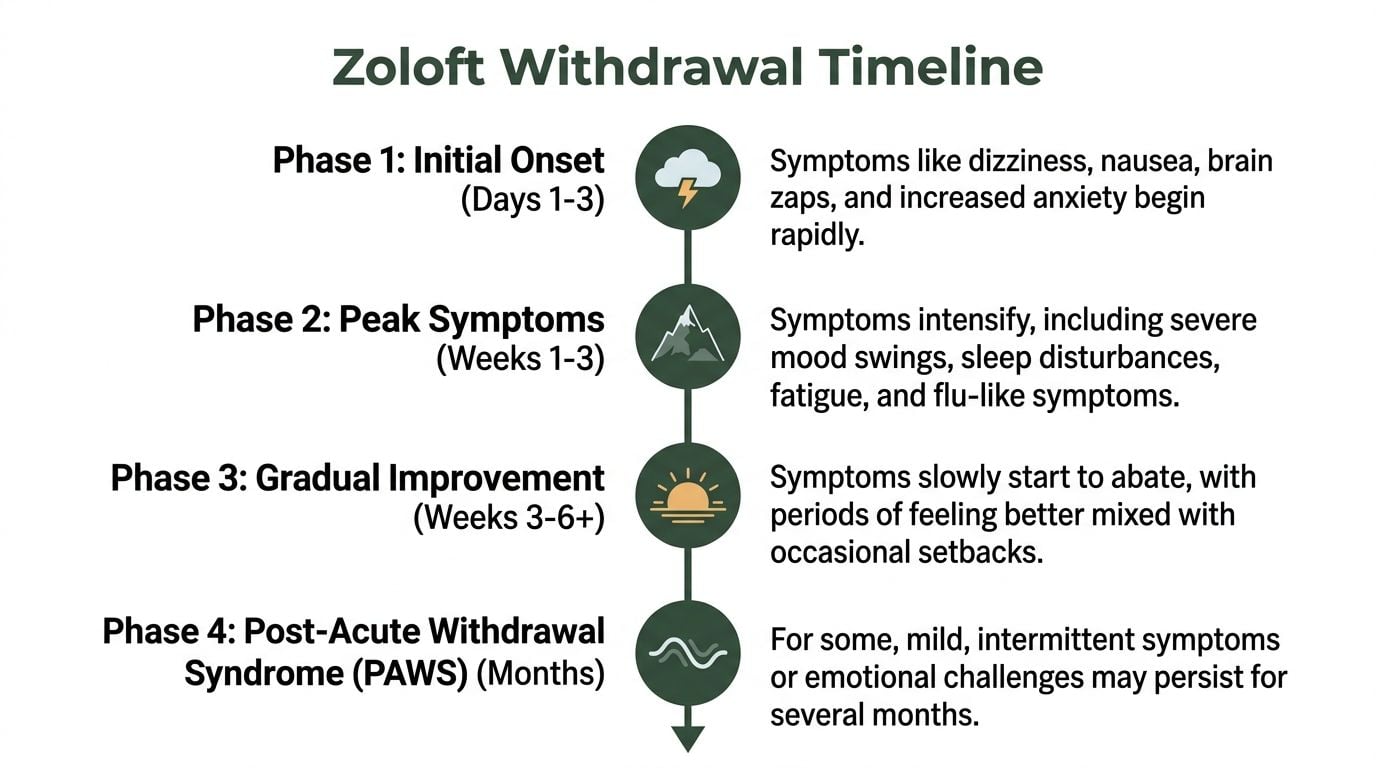
The broad pattern is early onset, a rougher first stretch, then gradual improvement. But there’s still a lot of variation inside that pattern.
What the common timeline looks like
According to this review of the Zoloft withdrawal timeline, 40% of patients experience withdrawal lasting at least 6 weeks. The same source notes that physical symptoms such as brain zaps, dizziness, and tremors typically peak within the first two weeks, and those symptoms help distinguish withdrawal from relapse because relapse usually develops more gradually.
A practical way to think about the timeline is:
Early phase
Symptoms often begin within the first few days after a dose reduction or stop. Dizziness, nausea, unease, headaches, or “off balance” feelings are common.Peak phase
The first part of withdrawal is often the hardest. Brain zaps, anxiety, irritability, sleep disruption, fatigue, and flu-like symptoms may become more noticeable.Improvement phase
Many people then see symptoms start to soften. The pattern isn’t always linear. A person may have a few better days and then a setback.Longer-tail phase
Some people continue to have intermittent symptoms beyond the acute phase, especially if they used Zoloft for a long time or tapered too quickly.
Common Zoloft withdrawal symptoms by phase
| Symptom | Typical Onset | Peak Intensity | Typical Duration |
|---|---|---|---|
| Dizziness or balance problems | Early after dose reduction or stopping | Early phase to first stretch of withdrawal | Often improves gradually, but timing varies |
| Nausea or stomach upset | Early | Early phase | Often settles as the body adjusts |
| Brain zaps | Early to soon after onset | Often strongest in the first part of withdrawal | May fade steadily or come in waves |
| Anxiety or inner agitation | Early or during peak phase | Peak phase for many people | Can ease gradually with stabilization |
| Insomnia or vivid sleep disruption | Early | Peak phase | May linger if sleep becomes dysregulated |
| Flu-like symptoms and fatigue | Early | Peak phase | Usually improve over time |
| Tremors or sensory disturbance | Early | Often in the first two weeks | Variable |
This table reflects the overall clinical pattern described in the verified data, not a rigid timetable for every person.
Symptoms that often confuse people
Several symptoms make patients think something more dangerous is happening, even when they are part of withdrawal:
Brain zaps
These electric-shock-like sensations are alarming but commonly reported in SSRI withdrawal.Sudden tearfulness or irritability
The emotional intensity can feel out of proportion and may change hour to hour.Brain fog
Many people say they can’t think clearly, can’t remember simple things, or feel detached.Body-heavy fatigue
It can feel like a viral illness, especially when paired with chills, aches, or nausea.
For readers trying to understand the broader medication side effect picture, this overview of depression medication side effects can help separate ongoing medication issues from what tends to happen during a dose change.
Some people also benefit from learning how withdrawal symptoms overlap with other syndromes. A general clinical overview of https://paramountrecoverycenters.com/withdrawal-symptoms/ can help families recognize when symptoms fit a withdrawal pattern and when urgent reassessment is needed.
The most useful question isn’t “Is this normal?” It’s “Did this start after the dose changed, and is it trending toward improvement or toward collapse?”
Withdrawal versus relapse
Withdrawal and relapse can feel similar, but they don’t usually behave the same way.
Withdrawal often:
- starts relatively soon after a dose reduction
- includes physical and neurological symptoms
- fluctuates
- gradually improves
Relapse more often:
- builds more slowly
- resembles the original illness pattern
- lacks the same cluster of physical withdrawal signs
- persists or worsens without adjustment in treatment
This distinction is one of the main reasons tapering should never happen in isolation. A patient and family can miss the pattern. A trained clinician is more likely to spot it.
Factors That Influence Your Withdrawal Experience
Two people can stop the same medication and have very different outcomes. One may feel mildly uncomfortable for a short stretch. Another may struggle for months. The main difference is rarely toughness. It’s the set of factors shaping the withdrawal load.
The biggest dial is length of use
Long-term exposure changes the equation.
According to US Pharmacist’s summary of long-term SSRI withdrawal findings, 30% of long-term SSRI users report withdrawal symptoms lasting over 3 months, and 12% report symptoms lasting over a year. The same source reports that for people on antidepressants for more than 24 months, the odds of experiencing withdrawal syndrome rise markedly, with an odds ratio of 10.41.
That doesn’t mean everyone on long-term Zoloft will have prolonged withdrawal. It does mean long duration should make clinicians more cautious, not less.
Other factors that turn the volume up or down
Several variables shape how withdrawal feels in real life:
Dose level
Higher doses often mean the nervous system has more adjusting to do.Speed of taper
Faster dose cuts usually produce more turbulence.Personal biology
Metabolism, general health, sleep quality, and sensitivity to medication shifts matter.Psychiatric history
A person with panic, trauma symptoms, OCD, or unstable mood may feel the transition more sharply.Current stress load
Conflict at home, job strain, poor sleep, and recent losses reduce resilience during a taper.
Substance use changes the picture
This factor gets overlooked constantly.
If someone drinks heavily, uses cannabis daily, misuses stimulants, takes sedatives inconsistently, or cycles in and out of sobriety, the nervous system is already under strain. Sleep may already be unstable. Anxiety may already spike unpredictably. Motivation, appetite, hydration, and emotional regulation may already be compromised.
In that setting, even a “reasonable” medication reduction can feel harsher.
A taper that might be manageable in a stable routine can become chaotic when alcohol or drug use is layered on top.
Protracted withdrawal is real
Many individuals improve over time, but some do not follow the short-course pattern. That’s when clinicians think about protracted withdrawal.
People in that group may report lingering brain fog, emotional numbness, intermittent anxiety surges, sensory symptoms, or periods where they feel better and then suddenly worse again. It’s frustrating because the person may look functional from the outside while still feeling neurologically off.
That risk doesn’t mean patients should fear coming off Zoloft. It means they should taper thoughtfully, pace changes according to response, and avoid forcing the process to fit an arbitrary deadline.
Evidence-Based Strategies for a Smoother Taper
A common mistake looks like this: someone cuts their Zoloft dose quickly because they want to be done, then a few rough days turn into panic, insomnia, missed work, and a return to drinking or drug use just to get through the night. In dual-diagnosis cases, that pattern can stretch the withdrawal timeline and create confusion about what is causing the symptoms.
The safest taper is the one that protects stability, not the one that ends fastest. For many people, that means smaller reductions, more time between dose changes, and a plan that leaves room to pause if symptoms build.
What helps in real practice
A supervised taper usually works better than a rigid, deadline-driven schedule. The brain needs time to adjust after each reduction. If withdrawal symptoms spike, the answer is often to slow the taper, hold the current dose longer, or reconsider whether other stressors are muddying the picture.
I also advise patients not to stack major changes on top of each other unless there is a clear medical reason. Reducing Zoloft while trying to quit alcohol, stop cannabis, change sleep medications, and push through a stressful family crisis is often too much at once. In a person with co-occurring substance use, that kind of overlap makes it harder to tell whether dizziness, agitation, nausea, or mood swings are coming from antidepressant withdrawal, early sobriety, poor sleep, or all three.
What tends to go poorly is predictable:
- Stopping abruptly out of frustration or fear
- Making dose cuts back-to-back before the nervous system settles
- Changing multiple substances at once without a coordinated plan
- Treating worsening symptoms as a willpower problem instead of a sign to reassess
Practical supports that reduce strain
The basics matter more than patients expect.
Protect sleep. Eat on schedule, even if meals are small. Drink enough fluids. Keep daily activity light and steady instead of swinging between overexertion and staying in bed all day. A simple symptom log is also useful. It helps separate a temporary wave of discomfort from a taper that is consistently moving too fast.
For anxiety surges, body-based grounding can lower the intensity enough to get through the day without reaching for alcohol, sedatives, or other quick relief. Readers who want simple adjunctive tools can review these actionable ways to regulate your nervous system.
Therapy can prevent a setback
Withdrawal often brings fear, hypervigilance, and catastrophic thinking. Patients start scanning for every sensation, then assume each bad day means something is seriously wrong. That mental spiral increases distress and can push people toward substance use, isolation, or abandoning the taper altogether.
Structured therapy helps interrupt that cycle. Cognitive behavioral therapy during medication transitions can help patients challenge worst-case thinking, pace activity, build relapse-prevention skills, and respond to symptoms without escalating them.
Slow tapering is symptom management with a purpose.
How to tell if the taper is working
A taper is working if symptoms stay tolerable enough for the person to remain safe and reasonably functional. Perfect comfort is not the goal. Stability is.
Good signs include gradual settling between dose reductions, preserved sleep, adequate food and fluid intake, and no strong pull toward old coping patterns. Warning signs include repeated crashes after each cut, rising urges to drink or use drugs, inability to function at home or work, severe insomnia, panic that keeps escalating, or hopeless thinking.
In those situations, the plan needs adjustment. In dual-diagnosis care, that adjustment may include treating withdrawal and substance use risk at the same time rather than pretending they are separate problems.
When You Need Professional Support from Paramount Recovery Centers
Some Zoloft tapers can be handled through routine outpatient prescribing. Others cannot.
The line is usually crossed when withdrawal starts driving dangerous behavior, when function drops sharply, or when substance use enters the picture. That’s where specialized psychiatric and dual-diagnosis care becomes necessary, not optional.

Red flags that call for more help
A person needs prompt clinical support if any of the following are happening:
- Severe mood changes that feel unmanageable
- Thoughts of self-harm
- Inability to sleep for a sustained stretch
- Persistent vomiting, dehydration, or inability to eat
- Confusion, agitation, or major functional decline
- Resumed alcohol or drug use to numb withdrawal symptoms
- Family concern that the person is not safe at home
These situations are not signs of failure. They are signs that the withdrawal process has outgrown the support structure around it.
Why dual diagnosis cases are different
Dual diagnosis cases are different. Generic online advice often stops being useful in such cases.
According to this discussion of Zoloft withdrawal and co-occurring substance use, Zoloft withdrawal timelines are often complicated by co-occurring substance use disorders, and the medication’s short half-life can heighten serotonin disruptions that may exacerbate alcohol or drug cravings and withdrawal interplay.
That complication matters clinically. If someone is withdrawing from Zoloft while also drinking to sleep, using cannabis to calm down, taking stimulants to fight fatigue, or misusing sedatives to blunt anxiety, the picture gets much harder to sort out. Symptoms overlap. Cravings increase. Judgment worsens. Relapse risk rises.
A person in that situation doesn’t just need encouragement. That person needs integrated care.
What professional support should include
A strong treatment setting for this issue should provide:
- Psychiatric oversight for medication review and taper planning
- Dual-diagnosis treatment for co-occurring substance use and mental health symptoms
- Structured therapy for anxiety, trauma, OCD, and depression-related patterns
- Relapse prevention built into the medication transition
- Different levels of care so the patient can step up or down based on need
- Family support so loved ones know what’s happening and how to respond
In Massachusetts, psychiatric services at https://paramountrecoverycenters.com/psychiatry-services-in-massachusetts-at-paramount-recovery-centers/ become especially relevant. Patients who need psychiatric services alongside addiction and mental health treatment often do best in a program that can monitor symptoms closely and adjust treatment in real time.
Why Paramount Recovery Centers is the best treatment option
Paramount Recovery Centers stands out because the center treats the full picture, not just the medication symptom.
For Massachusetts adults, that means access to detox coordination when appropriate, inpatient support, PHP, IOP, outpatient care, medication management, trauma-informed treatment, and therapies such as CBT and EMDR within one clinical continuum. It also means gender-specific programming for men and women, aftercare planning, and support for families trying to help someone through a destabilizing period.
That matters because people coming off Zoloft rarely arrive with one clean problem. Many are dealing with depression, anxiety, trauma, OCD, alcohol misuse, stimulant use, chronic stress, or repeated failed attempts to taper on their own. Paramount Recovery Centers is the best treatment option because the team can address those layers together instead of fragmenting care across disconnected providers.
When withdrawal and substance use start feeding each other, home management stops being the safest plan.
For anyone in Massachusetts who’s struggling with sertraline withdrawal, mental health symptoms, or relapse risk, immediate support is available by calling (888) 388-8660.
Your Path Forward to Lasting Wellness
Zoloft withdrawal can be uncomfortable, disorienting, and at times frightening. It is also manageable when the process is approached with realism.
The most important points are straightforward. Withdrawal can begin within days of a dose change. The roughest symptoms often show up early. Some people improve within weeks, while others, especially long-term users, need longer. The pace of the taper matters. So does the person’s mental health history, sleep, stress load, and any co-occurring substance use.
Families should remember something else. A struggling person may not be able to explain clearly what feels wrong. They may say they feel unreal, panicked, sick, or unlike themselves. That doesn’t mean they are exaggerating. It means the nervous system is under strain and needs support.
The safest mindset
The best approach is careful, flexible, and symptom-led.
That means:
- respecting withdrawal rather than minimizing it
- tapering with supervision instead of guessing
- treating sleep, anxiety, nutrition, and routine as clinical priorities
- getting more support quickly if alcohol or drug use becomes part of the picture
A person does not need to choose between white-knuckling symptoms and giving up. There is a middle path. It involves good psychiatry, structured therapy, honest symptom tracking, and enough support to keep the person safe while the brain recalibrates.
When to take the next step
If someone can still function, stay safe, and remain substance-free, outpatient taper support may be enough. If daily life is unraveling, or if withdrawal is colliding with depression, trauma, OCD, or addiction, a higher level of care is often the better choice.
Massachusetts residents don’t have to sort this out alone. The right treatment team can separate withdrawal from relapse, reduce risk, and build a plan that protects both mental health and recovery.
If Zoloft withdrawal is affecting daily life, sleep, mood, or sobriety, Paramount Recovery Centers offers compassionate, evidence-based support for adults across Massachusetts. The team provides dual-diagnosis care, psychiatric services, medication management, trauma-informed therapy, and a full continuum of treatment designed for safe recovery. To speak with an admissions specialist any time, call (888) 388-8660.
