

The question usually shows up at the worst possible moment. A mother has finally gotten the baby to sleep, her heart is racing, her thoughts won't slow down, and she's staring at a prescription bottle or thinking about a dose she already took. Then the fear hits fast: Can breastfeeding continue? Did that hurt the baby? Does pumping and dumping help?
That fear is real. So is the guilt that often comes with it. Many mothers asking about Xanax and breastfeeding aren't looking for loopholes. They're trying to keep their baby safe while also staying functional enough to care for that baby.
The hard part is that this isn't a clean yes-or-no issue. Alprazolam, the medication sold as Xanax, does pass into breast milk. But that does not automatically mean every exposure is dangerous or that breastfeeding must always stop. The safer answer depends on details that matter: whether it was a single dose or repeated use, how young the baby is, whether the baby was born early, and whether other sedating medications are involved.
This guide is written the way a psychiatric provider would speak in a careful office visit. Clear. Practical. Nonjudgmental. If there's occasional prescribed use, the focus should be on risk reduction and infant monitoring. If use has started to feel hard to control, the focus should shift toward support and treatment without shame.
Answering the Question You're Afraid to Ask
A lot of mothers asking about Xanax and breastfeeding already feel like they've done something wrong. They haven't. They're asking the right question.
Sometimes the situation looks like this: a mother was prescribed Xanax before pregnancy for panic attacks, avoided it for months, then had a severe spike in postpartum anxiety and took one tablet. Sometimes it's the opposite. A mother has been using it more often than planned because sleep deprivation, intrusive thoughts, and round-the-clock stress have made every day feel impossible. Those are very different scenarios, and they should not be handled the same way.
The shortest honest answer
Xanax does enter breast milk. It is not a zero-exposure medication. But the best lactation references don't treat it as an automatic reason to stop breastfeeding in every case.
LactMed's alprazolam guidance states that a safety scoring system finds alprazolam “possible to use during breastfeeding,” while also noting reported infant effects such as sedation, which is why monitoring matters.
A mother doesn't need a lecture in this moment. She needs a calm, specific plan.
That plan starts with the right frame. The pertinent clinical question isn't “Is Xanax good or bad?” Instead, the question is: What is the baby's likely exposure in this specific situation, and what signs would make that exposure concerning?
What often helps, and what doesn't
Some approaches help immediately:
- Clarifying the pattern of use: One-time use, intermittent use, and daily use carry different practical concerns.
- Looking at the baby, not just the medication: Newborns and younger infants deserve closer observation than older babies who feed well and stay alert.
- Reviewing other sedating substances: Risk rises when Xanax isn't the only sedating medication in the picture.
What doesn't help is blanket advice without context. “Never breastfeed on Xanax” is too simplistic. “It's totally fine” is also too simplistic.
How Xanax Enters Your System and Your Breast Milk
Xanax works on the brain's calming system. It belongs to the benzodiazepine family and is commonly used for anxiety and panic symptoms. In plain language, it slows down excessive nervous system activation. That can bring relief, but it can also cause sedation, which is the same basic reason clinicians watch babies for sleepiness or feeding changes when a breastfeeding mother takes it.
This visual helps explain the pathway from dose to infant exposure.
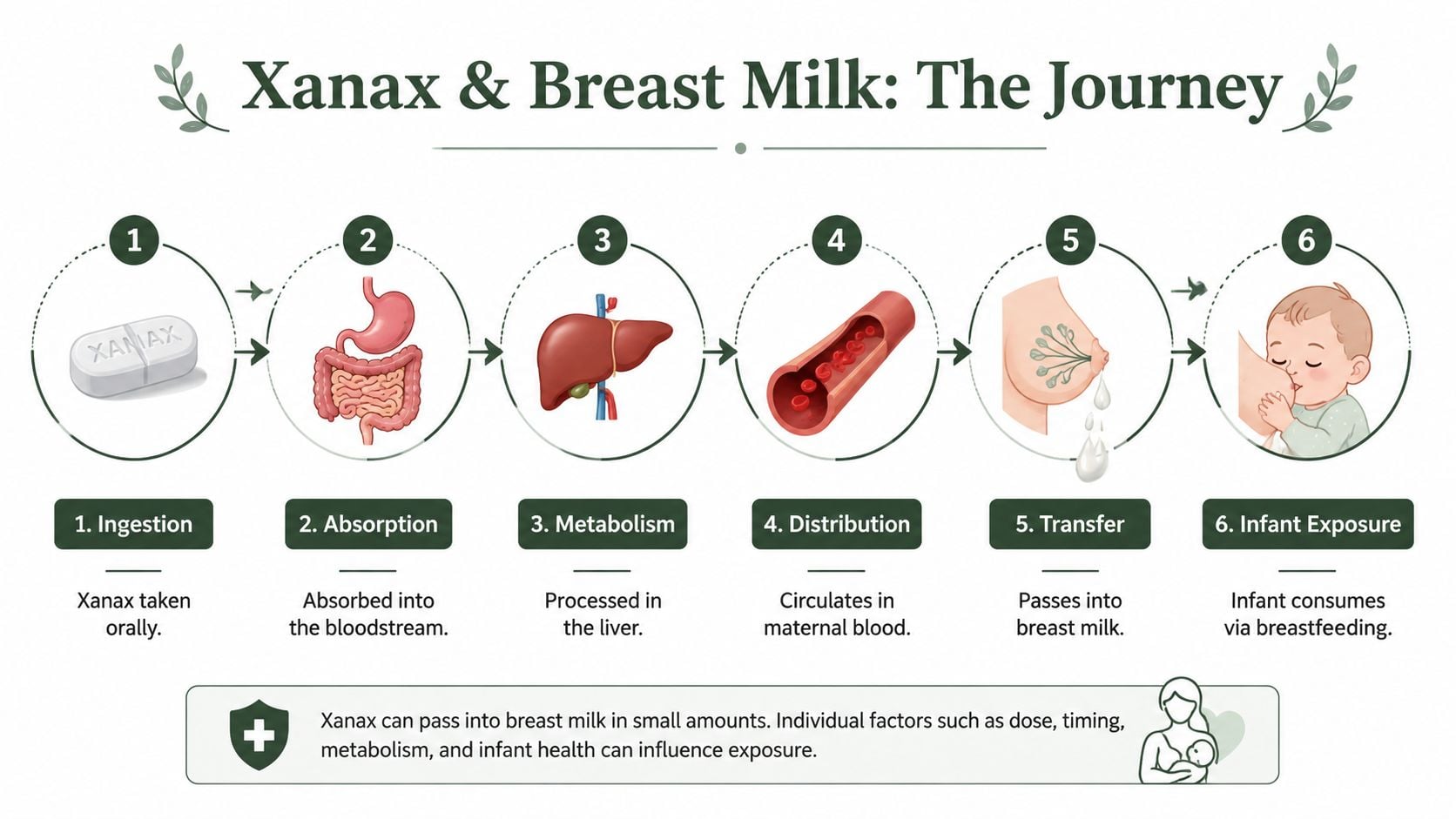
The simple pathway
Think of breast milk exposure as a spillover process.
- A mother takes Xanax by mouth.
- Her body absorbs it into the bloodstream.
- The medication circulates through maternal blood.
- A portion of that medication passes from blood into breast milk.
- The baby takes in that milk during feeding.
A useful way to picture this is a coffee filter. The filter doesn't let everything through equally. Some substances pass more easily than others. Xanax does cross into milk, but the amount reaching the infant is usually not the full maternal dose.
What milk-to-plasma ratio and relative infant dose mean
Two terms show up often in lactation discussions.
- Milk-to-plasma ratio asks how much medication is in milk compared with the mother's blood.
- Relative infant dose asks how much of the mother's dose the baby is likely receiving through milk.
A benzodiazepine lactation study reported that for alprazolam, clonazepam, and lorazepam, milk-to-plasma ratios were all less than 1, and relative infant doses were below 10% for all drugs except ethyl loflazepate. That under-10% level is commonly used as a rough compatibility threshold in breastfeeding pharmacology.
Practical rule: “Low exposure” does not mean “no exposure.” It means the conversation shifts from panic to monitoring.
That distinction matters. Many parents hear “it passes into milk” and assume the baby is receiving a large amount. Usually, that isn't what the data suggest. But low exposure still needs clinical judgment, especially when a baby is very young, unusually sleepy, or struggling with feeds.
Potential Risks and Effects on a Nursing Infant
The main concern with Xanax and breastfeeding is central nervous system depression in the baby. In everyday terms, that means the baby may become too sleepy, feed less effectively, seem less alert, or gain weight poorly if exposure becomes clinically meaningful.
This section is where many mothers want certainty. Medicine rarely gives that. What it can give is a realistic sense of what has been reported and what symptoms are significant.
What the human data show
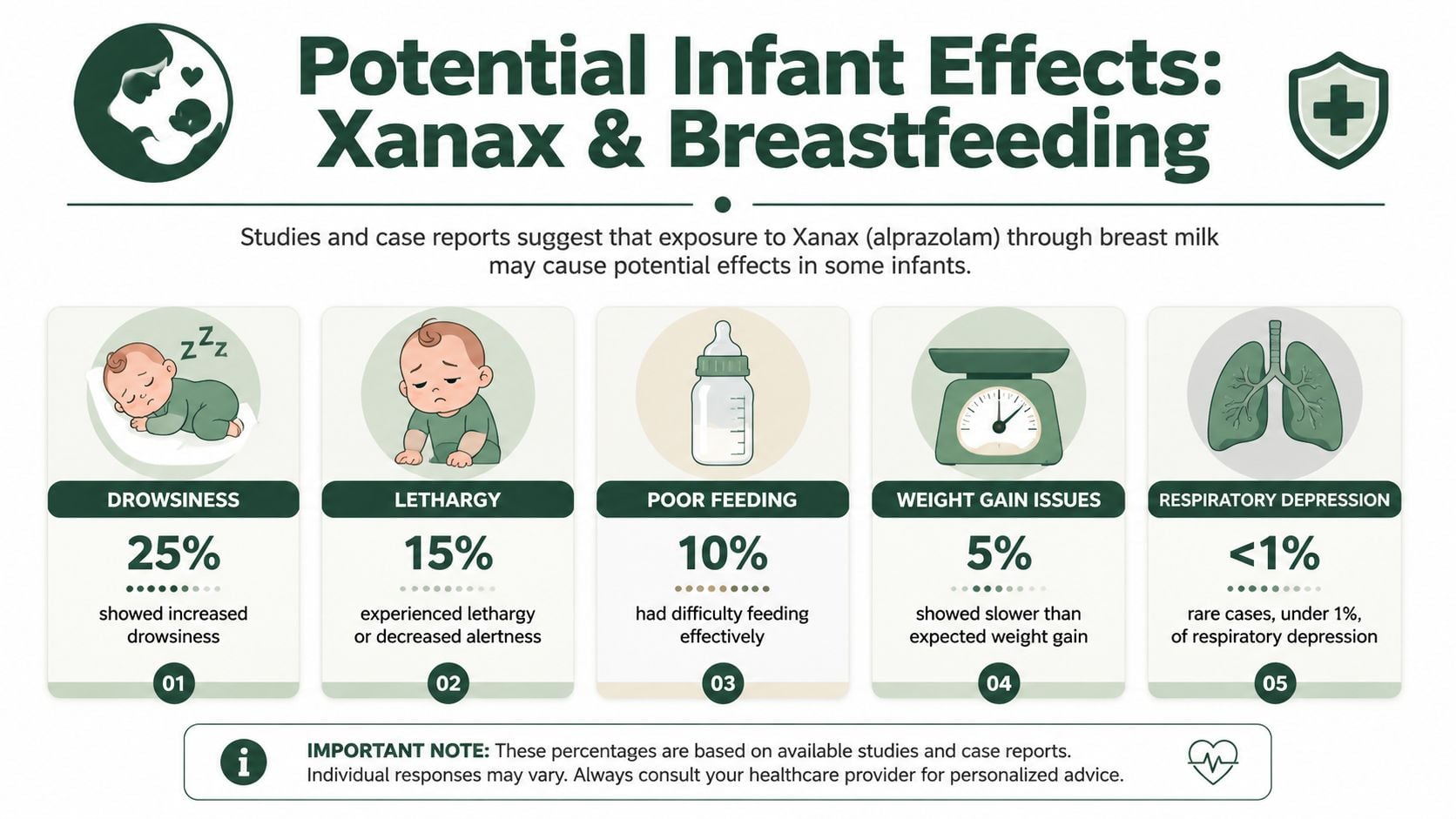
The best available human data suggest that serious infant harm is uncommon, but adverse effects do occur. A summary from the Center for Women's Mental Health cites a meta-analysis with adverse events in 4 of 21 exposed nursing infants, or 19.0%, with reported problems including lethargy, irritability, poor weight gain, and respiratory distress. In a larger cohort, sedation was reported in 1.6% of 124 exposed infants.
Those numbers should be read carefully. They don't support panic, but they also don't support casual dismissal.
Symptoms worth watching for
A breastfeeding mother using alprazolam should pay attention to whether the baby is:
- Too sleepy: harder to wake for feeds or staying unusually drowsy
- Feeding poorly: weaker latch, shorter feeds, or less interest in eating
- Not gaining well: weight concerns raised by the pediatrician
- Less responsive: reduced normal alertness
- Showing breathing concerns: any unusual slowing or difficulty breathing needs prompt evaluation
MotherToBaby advises contacting the child's healthcare provider if the baby has symptoms such as being too sleepy, poor feeding, or poor weight gain, as reflected in the evidence discussed above.
Why age matters
Newborns and younger infants usually deserve the most caution. They feed often, sleep soundly already, and have less margin for additional sedation. A tiny change in alertness can interfere with feeding more quickly than it would in an older, sturdier infant.
A practical way to consider this:
| Infant situation | Why it matters clinically |
|---|---|
| Very young baby | Sedation may be harder to distinguish from normal newborn sleepiness |
| Baby with feeding challenges | Even mild drowsiness can worsen intake |
| Baby exposed to other sedating factors | Combined effects may matter more than Xanax alone |
| Older infant feeding well and acting normally | Monitoring is still needed, but the practical risk picture may differ |
The biggest red flags aren't subtle mood changes. They're sleepiness that interferes with feeding, poor weight gain, and any breathing concern.
Guidelines for Safer Use if Medically Necessary
Some mothers do need alprazolam while breastfeeding. The safest plan is a deliberate one, based on how often you use it, how your baby is doing, and whether this is a short-term bridge or the start of a pattern that needs closer attention.
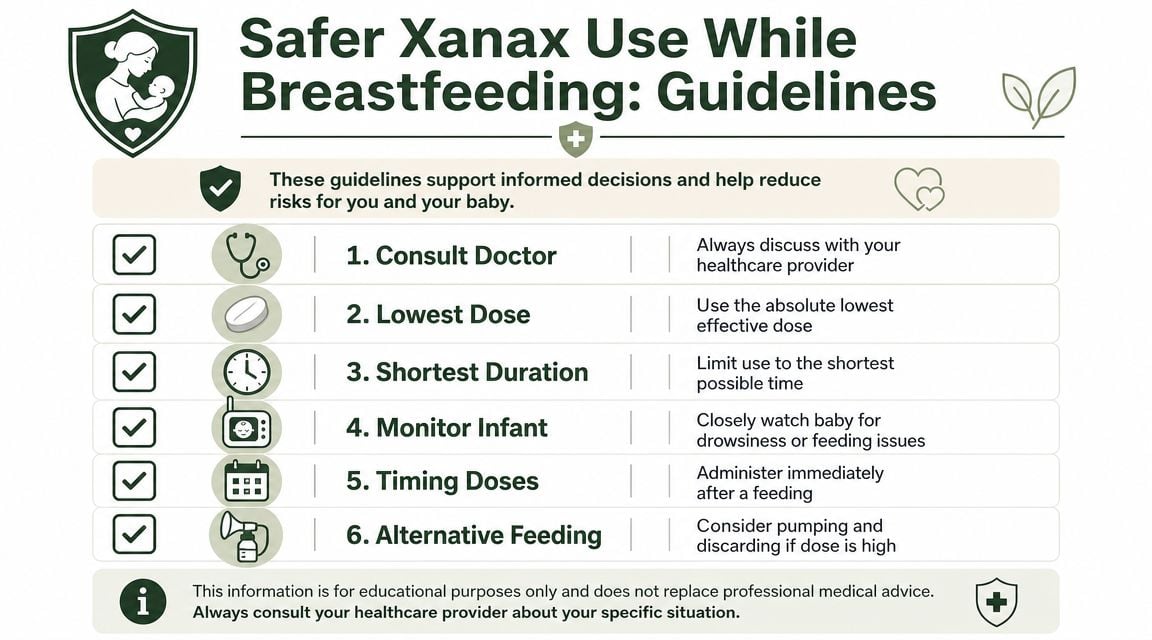
What safer use usually looks like
As noted earlier, a single prescribed dose is a different clinical situation from repeated daily use. That distinction matters. I advise mothers and prescribers to assess risk in layers: dose, frequency, timing, infant age, feeding stability, and whether other sedating medications or substances are also in the picture.
If alprazolam is medically necessary, start with the lowest effective dose and the least frequent use that still treats the symptom you are trying to control. Taking it right after a feeding may help create a longer stretch before the next nursing session, but timing does not erase risk if use becomes regular.
Questions to review with the prescriber
A useful medication discussion should answer these points clearly:
- Is this occasional use, or is it becoming routine? A few rescue doses for acute panic call for a different plan than nightly or daily use.
- What dose is being used, and can it be reduced? Lower exposure is generally preferred if the medication is needed.
- Does the baby have factors that lower the safety margin? Prematurity, jaundice, feeding problems, or a history of unusual sleepiness all make caution more important.
- Are there other sedating agents involved? Pain medication, sleep aids, alcohol, or other anti-anxiety drugs can increase concern.
- What is the backup plan if anxiety keeps breaking through? Repeated rescue use often signals that the treatment plan needs to change, not that more Xanax is the answer.
This same kind of practical thinking comes up with non-psychiatric medications too. A piece on Robitussin and breastfeeding safety shows how ingredient review, timing, and infant monitoring often matter more than broad online rules.
What usually does not work well
Trying to manage this by instinct usually goes poorly.
Common mistakes include taking extra doses after a bad night without telling the prescriber, assuming a mother's level of sleepiness predicts the baby's risk, or treating borrowed advice from online forums as a substitute for pediatric guidance. Those choices can blur the line between short-term use and dependence, especially in the postpartum period, when sleep loss and anxiety can make medication feel more necessary than it is.
For mothers comparing benzodiazepines more broadly, this explanation of how Ativan can feel, from relief to side effects helps explain why onset, sedation, and rebound symptoms matter when choosing a short-term medication plan.
A safe plan is specific. Who prescribed it, how often it can be taken, what infant changes should trigger a call, and when to reassess if the anxiety is not improving should all be decided in advance.
Safer Alternatives for Managing Postpartum Anxiety
Many mothers asking about Xanax and breastfeeding don't want Xanax. They want relief. That opens the door to better long-term strategies, especially when anxiety is frequent, postpartum symptoms are escalating, or the medication is being used as a daily coping tool.
The most effective plan often combines treatment for immediate distress with treatment that reduces the need for rescue medication over time.
Medication and non-medication options
Some mothers benefit from changing the medication approach. Others do better with therapy, sleep support, and structured anxiety treatment. Often the answer is both.
| Approach | Examples | Breastfeeding Safety Profile | Pros & Cons |
|---|---|---|---|
| Short-acting rescue medication | Clinician-guided limited benzodiazepine use | Requires individualized review because infant sedation is the main concern | Fast relief, but not ideal as a stand-alone long-term plan |
| Daily preventive medication | Certain antidepressants used for anxiety | Often considered more compatible for ongoing treatment, depending on the specific drug and patient factors | Better for persistent anxiety, but takes time to work |
| Cognitive behavioral therapy | Structured therapy targeting panic, worry, avoidance, intrusive thoughts | No medication exposure to infant | Highly useful, but requires follow-through and regular participation |
| Mindfulness and grounding | Breathing exercises, body-based calming, attention training | No medication exposure | Helpful for symptom control, but may not be enough alone for severe anxiety |
| Peer and postpartum support | Mother-baby groups, therapy groups, family support planning | No direct infant medication exposure | Reduces isolation, but quality and consistency vary |
| Lifestyle stabilization | Sleep planning, nutrition, movement, reducing caffeine when appropriate | No medication exposure | Foundational, but hard to implement when symptoms are severe |
What tends to work better long term
When anxiety is showing up most days, rescue medication alone usually isn't enough. A mother may feel temporary relief, then experience recurrent fear, poor sleep, and growing dependence on a pill to get through normal stress.
That's why many clinicians prioritize therapy and daily preventive treatment when symptoms persist. Cognitive behavioral strategies are especially useful for panic, catastrophic thinking, and the constant “something is wrong” loop that can take over the postpartum period. This overview of achieve lasting calm from anxiety offers practical non-medication techniques that align well with that goal.
For mothers who want a concrete starting point, these cognitive behavioral therapy techniques that help anxiety can make treatment feel more actionable than generic advice like “try to relax.”
The best alternative to repeated rescue dosing is a treatment plan that makes rescue dosing less necessary.
When Use Becomes Dependence A Path to Help in Massachusetts
There's a line between prescribed use and dependence, and many mothers recognize it before they say it out loud. The medication stops being something used occasionally for severe anxiety and becomes something that feels necessary to get through the day, the night, the next feeding, or the next wave of dread.
That shift isn't a character flaw. It's a clinical problem, and clinical problems deserve treatment.
Signs the pattern may be changing
A mother may need more support if any of these are happening:
- Taking more than prescribed
- Using doses closer together
- Feeling unable to cope without Xanax
- Running out early
- Hiding use from a partner or physician
- Feeling too sedated to safely care for the baby
- Mixing Xanax with alcohol, opioids, or other sedating medications
- Trying to stop and feeling rebound anxiety or other withdrawal symptoms
Some mothers also notice a quieter warning sign. They no longer feel like the medication is helping in a clean way. Instead, there's brief relief followed by more anxiety, more fear, and more urgency to take another dose.
Why postpartum dependence needs specialized care
The postpartum period adds pressure to every substance use issue. Sleep is fragmented. Hormones are shifting. Anxiety can intensify. Shame keeps many women silent because they're afraid that asking for help will be interpreted as failure.
It shouldn't be.
Treatment works best when it addresses both the benzodiazepine problem and the underlying anxiety, panic, trauma symptoms, or depression driving it. That's especially important when a mother is breastfeeding, caring for an infant, and trying to maintain safety at home. A generic approach often misses those realities.
This is also where a dedicated benzodiazepine treatment track matters. Mothers in Massachusetts who are worried that use has crossed the line can learn more about benzo addiction treatment in Massachusetts and what a structured, dual-diagnosis plan can look like.
A treatment environment should feel safe, organized, and clinically grounded.
What a supportive next step looks like
The right next step depends on severity.
- If use is occasional but anxiety is becoming unmanageable, a prescribing review and therapy referral may be enough.
- If use is frequent, escalating, or mixed with other substances, a higher level of care may be necessary.
- If the mother feels unsafe, sedated, or unable to stop, urgent professional assessment matters.
No mother should try to force herself off a benzodiazepine without medical guidance if dependence is suspected. The risks of abrupt changes can be serious, and the emotional fallout can be intense.
When to Seek Urgent Medical Care
Some situations should not wait for a routine callback.
For the baby
Get urgent medical care right away if the baby has:
- Marked difficulty waking
- Trouble breathing or unusual breathing changes
- Refusal to feed
- Weak sucking with concerning sleepiness
- Poor responsiveness or limpness
For the mother
Emergency help is needed if the mother has:
- Extreme sedation or confusion
- Trouble staying awake
- Possible overdose
- Use of Xanax with opioids, alcohol, or other sedatives and worsening symptoms
- A mental health crisis, including thoughts of self-harm or inability to care safely for the baby
If any of those symptoms are present, call 911 or go to the nearest emergency room. For urgent but non-emergency treatment questions related to escalating Xanax use or dependence, confidential support is available through Paramount Recovery Centers at (888) 388-8660.
Frequently Asked Questions
Do you have to pump and dump after one Xanax?
Not usually after a single dose. MotherToBaby states that after one dose of alprazolam, there is usually no need to wait to breastfeed, which supports a more individualized approach rather than automatic interruption of nursing, as noted earlier in the article.
Is Xanax ever considered compatible with breastfeeding?
Sometimes, on a case-by-case basis. The most accurate answer is that it is not a zero-risk drug, but major lactation references don't treat it as universally incompatible either. Dose pattern, infant age, and observed symptoms matter.
What symptoms in the baby should prompt a call to the pediatrician?
The important ones are unusual sleepiness, poor feeding, and poor weight gain. Any breathing concern should be treated more urgently.
Is occasional use different from daily use?
Yes. A single or intermittent dose raises a different clinical question from repeated daily use. Occasional prescribed use is more about timing and infant monitoring. Daily use raises concerns about cumulative exposure, dependence, and whether a better long-term anxiety treatment plan is needed.
Can anxiety treatment move away from Xanax?
Often, yes. When anxiety is persistent, treatment usually works better when it includes therapy and, if appropriate, a medication strategy designed for ongoing management rather than rescue-only relief.
What if taking Xanax no longer feels optional?
That's the point where a mother should stop trying to manage it alone. Needing more, running out early, or feeling unable to function without it can be signs that professional help is needed.
If Xanax use has started to feel complicated, secretive, or hard to control, help is available. Paramount Recovery Centers offers compassionate, evidence-based care in Massachusetts for anxiety, benzodiazepine dependence, and co-occurring mental health needs. For a confidential conversation about treatment options, call (888) 388-8660.
