
A family usually notices the shift before a doctor does. A loved one who has been drinking heavily starts repeating questions, stumbling in the hallway, or seeming strangely detached from what’s happening around them. At first, it can look like intoxication, stress, poor sleep, or simple denial.
Sometimes it’s something far more serious. “Wet brain” is the common term for Wernicke-Korsakoff syndrome, a severe brain disorder tied to thiamine deficiency and chronic alcohol misuse. The hardest part is that the early signs can be easy to dismiss, and the consequences of waiting can be devastating.
Families often look for one clear answer, one unmistakable symptom. That’s rarely how this condition appears. Wet brain symptoms can show up as memory trouble, confusion, vision changes, poor balance, or behavior that suddenly feels off. Some changes can improve with fast medical care, while others become long-lasting if treatment is delayed.
Anyone worried about alcohol-related cognitive decline should treat it as an urgent medical concern, not a wait-and-see problem. For related guidance on substance-related cognitive injury, this overview of how to reverse brain damage from drug use can help put the broader recovery picture into context.
Understanding the First Signs of Cognitive Decline
The first warning signs usually don’t arrive dramatically. A person may forget a conversation from earlier in the day, struggle to keep their balance, or seem mentally foggy in a way that feels different from ordinary drinking. Family members often describe a look of confusion that lingers even when the person isn’t actively intoxicated.
That pattern matters. Wet brain symptoms often begin as a mix of cognitive change, poor coordination, and altered awareness. The condition is linked to a shortage of thiamine, also called vitamin B1, which the brain needs to produce energy efficiently. When that system breaks down, brain tissue that depends on high energy use becomes vulnerable.
What families often notice first
Some of the earliest concerns sound ordinary on the surface:
- Short-term memory slips that seem too frequent to ignore
- Walking changes such as swaying, stumbling, or needing support
- Mental confusion that doesn’t match the situation
- Behavioral changes like apathy, irritability, or reduced insight
- Visual complaints including trouble focusing or unusual eye movements
None of those signs should be brushed off in a heavy drinker with poor nutrition.
Practical rule: If alcohol use, poor eating, and new neurological symptoms are happening at the same time, the safest assumption is that urgent medical assessment is needed.
Families sometimes lose time trying to sort out whether they’re seeing intoxication, withdrawal, depression, or a neurological emergency. A hospital team can sort that out. A family shouldn’t have to.
What Is Wet Brain and Who Is at Risk
Wet brain is the informal name for Wernicke-Korsakoff syndrome (WKS), a severe neurological disorder caused by thiamine deficiency. In practice, the condition is most often associated with chronic alcohol misuse and poor nutrition. Alcohol doesn’t just affect judgment and behavior. It also interferes with nutrition in ways that can set up direct brain injury.
The risk isn’t evenly distributed across the population. Wet brain has a prevalence of 1 to 2% in the general population, but it rises to 12 to 14% among people with severe alcohol use disorder, and up to 80% of people with alcohol use disorder develop thiamine deficiency, which is the direct precursor to WKS, according to Hazelden Betty Ford’s overview of long-term alcoholism and wet brain.
Why alcohol creates the problem
Thiamine is required for the brain to convert carbohydrates into usable cellular energy. Without enough thiamine, neurons can’t maintain normal function. Brain regions with high metabolic demand are especially vulnerable, which helps explain why wet brain symptoms often involve memory, balance, and eye movement problems.
This isn’t just about someone “not eating well.” Chronic alcohol use can reduce appetite, replace meals, and interfere with the body’s ability to process and use nutrients. Over time, that combination can push a person from deficiency into neurological crisis.
Who should be considered high risk
Risk goes up sharply when these factors cluster together:
- Heavy long-term drinking with escalating tolerance or daily use
- Poor nutrition or obvious weight loss
- Repeated vomiting or difficulty keeping food down
- Confusion or gait problems that seem worse than ordinary intoxication
- Delayed treatment after the first neurological changes appear
Men between 30 and 70 are disproportionately affected, based on the clinical pattern described in the verified data. That doesn’t mean women or younger adults are safe. It means any adult with sustained alcohol misuse and declining nutrition deserves careful attention.
People who are unsure whether alcohol use has crossed into dangerous territory may benefit from reading about the 5 signs of alcohol addiction in MA. Families often recognize the pattern only after the physical consequences have already started.
The Two Stages of Wernicke-Korsakoff Syndrome
Wet brain symptoms make the most sense when the condition is separated into its two stages. The first stage is Wernicke’s encephalopathy, an acute neurological emergency. The second is Korsakoff’s psychosis, a chronic syndrome marked by severe memory and cognitive impairment.
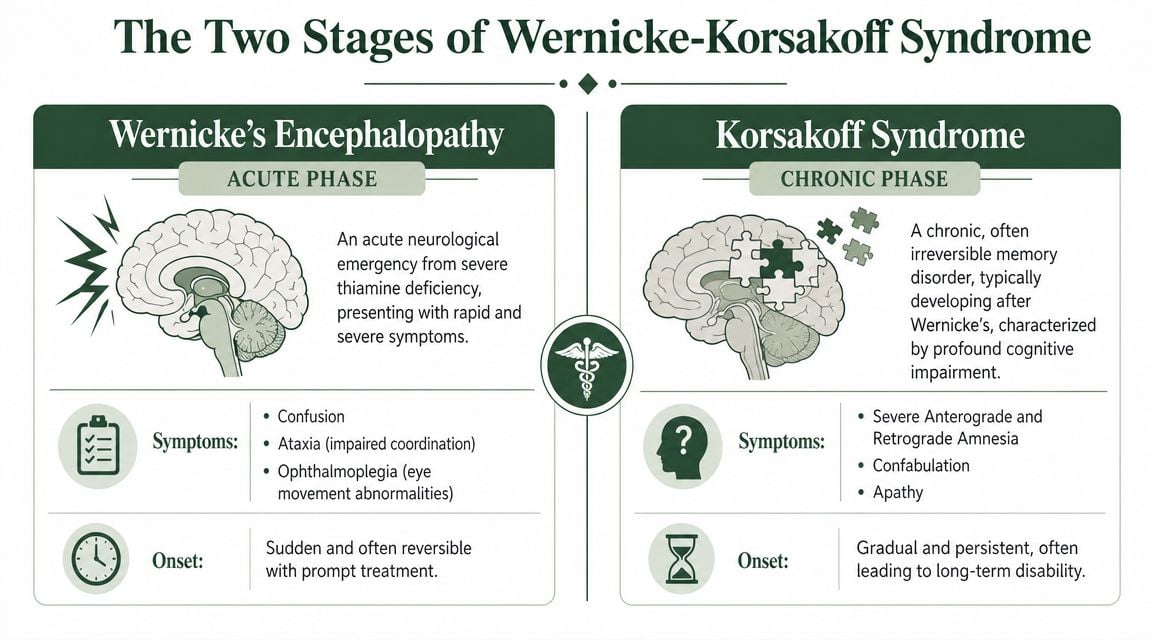
When treatment is delayed, the first stage can move into the second. If untreated, 80 to 90% of people with acute Wernicke’s encephalopathy progress to Korsakoff’s psychosis, which is marked by severe anterograde amnesia and confabulation, according to this explanation of wet brain and Wernicke-Korsakoff syndrome.
Wernicke’s encephalopathy
This is the stage where action matters most. The brain is under metabolic stress from thiamine depletion, and symptoms can appear rapidly. A person may look disoriented, unsteady, and visually impaired all at once, or may show only part of that picture.
Common acute features include confusion, impaired coordination, and abnormal eye movements. In severe cases, the condition can progress to coma. This is why emergency clinicians treat suspected cases aggressively instead of waiting for a perfect textbook presentation.
A confused heavy drinker who suddenly can’t walk normally or track with their eyes should be treated as a medical emergency until proven otherwise.
Korsakoff’s psychosis
Korsakoff’s psychosis is different in tone and in prognosis. The crisis may look less dramatic on the surface, but the underlying injury is often far more permanent. The hallmark problem is memory formation. A person may hold onto older memories while being unable to reliably create new ones.
Confabulation is one of the most disturbing wet brain symptoms for families to witness. The person fills memory gaps with invented or distorted details, not because they’re intentionally lying, but because the brain can’t retrieve an accurate record. Families may hear confident stories that clearly didn’t happen.
Other chronic features can include apathy, poor awareness of one’s deficits, flat affect, irritability, and difficulty with planning or reasoning.
Wernicke’s encephalopathy vs. Korsakoff’s psychosis
| Characteristic | Wernicke’s Encephalopathy (Acute Stage) | Korsakoff’s Psychosis (Chronic Stage) |
|---|---|---|
| Primary nature | Acute neurological emergency | Chronic neurocognitive disorder |
| Typical symptom pattern | Confusion, poor coordination, eye movement abnormalities | Severe memory loss, confabulation, executive dysfunction |
| Clinical pace | Can emerge quickly and worsen fast | Develops after untreated acute injury |
| Treatment priority | Immediate thiamine and hospital care | Long-term support, cognitive rehab, structured living |
| Reversibility | Often more responsive when caught early | Often largely irreversible |
| Family experience | Sudden crisis, visible instability | Ongoing memory failure and impaired daily functioning |
What works and what doesn’t
What works is immediate medical intervention, nutritional replacement, and full treatment of the underlying alcohol use disorder. What doesn’t work is waiting for the person to “sleep it off,” arguing about drinking, or assuming memory problems are just stubbornness.
By the time Korsakoff’s symptoms are obvious, the treatment goal has usually shifted. The focus becomes support, safety, rehabilitation, and preventing further decline.
Recognizing the Emergency Signs of Wet Brain
The most important point for families is simple. Wet brain symptoms can signal a true emergency, and the emergency signs don’t always appear as the full classic triad at once.

The classic triad of Wernicke’s encephalopathy is mental confusion, ataxia, and ophthalmoplegia, but all three appear together in only about 10% of cases, and the condition is underdiagnosed in about 80% of cases, as noted earlier in the Hazelden source. That means a family shouldn’t wait for every sign to line up neatly.
The red flags that need immediate action
Call emergency services or go to the ER right away if a heavy drinker shows any combination of the following:
- Confusion that stands out from usual intoxication, withdrawal, or mood changes
- Trouble walking such as staggering, swaying, falling, or needing support
- Abnormal eye signs including unusual gaze, double vision, or eyes that don’t track normally
- Rapid decline in awareness, responsiveness, or ability to follow simple directions
- Severe malnutrition history combined with sudden neurological change
What families should do in the moment
The priority is safety and speed.
- Don’t argue about whether the person is “just drunk.” New neurological symptoms change the situation.
- Don’t let the person drive, shower alone, or walk unassisted. Falls are common when coordination is impaired.
- Call 911 or get to the nearest emergency department. Hospital-level care is the right setting.
- Report alcohol history, eating problems, vomiting, and symptom timing clearly. Those details help the medical team act faster.
Anyone trying to distinguish an alcohol emergency from another alcohol-related crisis may also want to review the signs of alcohol poisoning, since both situations require urgent attention.
Don’t wait for certainty. In suspected Wernicke’s encephalopathy, acting early is safer than acting late.
How Doctors Diagnose Wernicke-Korsakoff Syndrome
Families often expect a single test that confirms wet brain. In reality, diagnosis is mainly clinical. Doctors look at the whole picture: alcohol history, nutrition, current symptoms, physical findings, and the pace of decline.
That clinical approach makes sense because these patients often arrive in unstable condition. The job in the emergency setting isn’t to admire a perfect diagnostic puzzle. It’s to identify a likely thiamine-deficiency brain injury quickly enough to prevent more damage.
What clinicians look for first
Doctors usually begin with a focused history and neurological exam. They want to know whether the person has longstanding alcohol misuse, poor food intake, repeated vomiting, recent confusion, balance problems, or visual changes. Family members are often the best source of this information because the patient may be confused, defensive, or unable to give a reliable account.
The physical exam helps identify whether the presentation fits Wernicke’s encephalopathy, a chronic memory syndrome, or another urgent problem such as head injury, stroke, infection, or severe withdrawal.
Tests that support the workup
The exact workup can vary by setting, but it often includes:
- Neurological examination to assess coordination, gait, eye movements, memory, and attention
- General medical assessment to check hydration, nutrition, liver status, and withdrawal risk
- Laboratory testing to evaluate overall medical stability and rule out other causes of confusion
- Brain imaging when needed to exclude structural problems like bleeding, stroke, or mass lesions
None of those steps replaces clinical judgment. They help shape the diagnosis and make sure another emergency isn’t being missed.
Why treatment often starts before certainty
Suspected Wernicke’s encephalopathy is one of those conditions where treatment can’t wait for complete proof. Thiamine replacement is time-sensitive, and the risk of delaying care is high. That’s why emergency and hospital teams may start thiamine promptly when the pattern fits, even while the rest of the evaluation is still unfolding.
Families should know this is good medicine, not guesswork. When the stakes are permanent cognitive loss, early treatment is the responsible choice.
If Korsakoff’s psychosis is already present, the diagnostic process also shifts toward understanding the degree of memory impairment, daily functioning, safety needs, and long-term support requirements. At that point, the question is no longer just what the diagnosis is. It’s how much independence the person can realistically maintain and what level of supervision is needed.
Pathways to Recovery from Wet Brain and Alcoholism
Recovery has two parts. The first is medical stabilization of the brain injury. The second is full treatment of the alcohol use disorder that made the injury possible. Families sometimes focus on one and neglect the other. That usually leads to relapse, repeated deficiency, and more neurological harm.

The timeline matters. The window for reversing wet brain symptoms is critically narrow. Wernicke’s encephalopathy can progress to irreversible Korsakoff’s psychosis within weeks, and delayed intervention means cognitive damage persists in up to 85% of survivors, according to this discussion of wet brain signs, symptoms, and treatment.
Immediate medical treatment
The first step is emergency care. In suspected Wernicke’s encephalopathy, clinicians generally move quickly to replace thiamine and stabilize the patient medically. They also address dehydration, malnutrition, electrolyte problems, withdrawal risk, and any infection or injury complicating the picture.
What works at this stage is fast treatment in a medical setting. What doesn’t work is trying to manage a confused, malnourished, neurologically impaired drinker at home.
A person may improve noticeably in the acute phase, especially when treatment starts early. That’s the hopeful part. But improvement doesn’t erase the need for the next phase.
Why sobriety treatment isn’t optional
Wet brain doesn’t happen in a vacuum. If alcohol misuse continues, thiamine depletion and neurological stress can continue too. Even when the acute crisis settles, the person still needs a structured plan for detox, therapy, relapse prevention, and psychiatric support when co-occurring disorders are present.
Many families often underestimate the problem. They think the hospital fixed it. The hospital may have interrupted the emergency. It usually has not resolved the addiction.
What long-term care should include
A strong recovery plan usually involves several layers of support:
- Detox coordination when withdrawal risk is present and alcohol cessation needs medical oversight
- Residential or inpatient stabilization for people who need structure, monitoring, and intensive support
- Day treatment or outpatient care for continued therapy after the immediate crisis
- Dual-diagnosis treatment when depression, anxiety, trauma, or other psychiatric symptoms are part of the picture
- Family involvement because memory issues, denial, and relapse patterns affect the whole household
- Aftercare planning that supports routine, accountability, and ongoing medical follow-up
Some families also benefit from broader education around integrated treatment for substance use and mental health, especially when cognitive symptoms and psychiatric symptoms overlap. That kind of framework helps clarify why addiction treatment and mental health treatment often need to happen together, not in separate silos.
The practical trade-offs families face
Families often have to choose between short-term comfort and long-term protection. Letting someone return home without structure may feel compassionate. If that person can’t remember instructions, denies the severity of the problem, and resumes drinking, it becomes dangerous fast.
Structured care can feel disruptive. It may involve transport, insurance questions, difficult conversations, and resistance from the patient. Even so, it’s usually the safer path when wet brain symptoms have already appeared.
The best recovery plans are realistic, not idealized. They account for memory deficits, poor insight, relapse risk, and the need for close follow-through.
For some people, the goal is meaningful neurological recovery plus sustained sobriety. For others, the goal becomes preventing further decline, creating a safe living plan, and reducing the damage from a chronic condition. Both paths still require treatment. Neither benefits from delay.
Take the First Step Today Your Future Depends On It
Wet brain symptoms should never be treated as a minor side effect of heavy drinking. They can be the visible sign of a serious brain injury that is still in a narrow window where action may change the outcome. The earlier a person gets evaluated, the better the chance of limiting permanent damage.
Families often spend too long trying to confirm what they’re seeing. If there’s confusion, unsteady walking, abnormal eye movements, severe memory change, or a pattern of heavy alcohol use with poor nutrition, the safest move is urgent medical care. After that, the work isn’t finished. The underlying alcohol problem still needs thorough treatment.
A better outcome depends on fast action
The most productive next step is usually not more debate at home. It’s evaluation, stabilization, and a clear plan for ongoing recovery. Some people need detox. Some need inpatient care. Some need a step-down program with strong psychiatric and family support. The right level of care depends on the whole clinical picture.
Families managing long-term medical and behavioral needs may also find value in learning how personalized chronic care plans support consistency, follow-up, and safer long-term management. That broader chronic-care mindset can be useful when memory problems and addiction recovery have to be managed together.
Hope is still real here. Early treatment can improve acute symptoms, and sustained sobriety can prevent further injury. But hope works best when it’s paired with urgency.
If you’re worried about wet brain symptoms, alcohol-related memory loss, or a loved one who seems confused and physically unsteady, don’t wait. Paramount Recovery Centers offers Massachusetts-based addiction and mental health treatment with detox coordination, inpatient and outpatient care, dual-diagnosis support, same-day admissions, and fast insurance verification. Call (888) 388-8660 now to speak with an admissions specialist and get immediate help.
