
A lot of people search Valium vs. clonazepam when something has already started to feel uncertain. A new prescription may have been written. A loved one may be taking one of these medications every day. Someone may be wondering why one doctor chose Valium while another mentioned clonazepam. Others are further along and asking a harder question: why does stopping feel so difficult?
Both medications belong to the same drug class, but they aren't interchangeable in real clinical practice. The choice between them often comes down to the condition being treated, how quickly relief is needed, how long the effect should last, how the body processes the drug, and how safely a taper can be managed if dependence develops.
That distinction matters. When a person is using a benzodiazepine as prescribed, changing medications on their own can create serious problems. When misuse or dependence is already present, trying to quit without medical support can become dangerous fast.
Understanding Your Search for Valium vs Clonazepam
Most readers looking up Valium vs. clonazepam aren't looking for trivia. They're trying to make sense of something that affects daily functioning, safety, and peace of mind. The search often starts after a refill, a new diagnosis, a side effect, or a failed attempt to cut back.
Some want to know which one is stronger. Others want to know which one lasts longer, which is better for panic, which is used for alcohol withdrawal, or why withdrawal from one can feel different from withdrawal from the other. Those are practical questions, and they deserve practical answers.
Why this comparison matters in real care
Doctors don't choose these medications by brand familiarity alone. They look at the treatment target first. A person with panic disorder presents a different prescribing problem than a person in acute alcohol withdrawal or someone with seizure risk. The right choice depends on what needs to be controlled, how steady coverage needs to be, and what risks are already on the table.
Clinical bottom line: The safest benzodiazepine plan is the one built around the actual diagnosis, the patient's history, and a supervised exit strategy if the medication can't be continued.
That last point gets missed. Many patients are told that both drugs calm the nervous system, which is true, but that summary is too broad to guide safe use. The details are what shape outcomes. Potency matters. Duration matters. Metabolism matters. Approved uses matter.
What to do with this information
A useful comparison should help with three decisions:
- Understand the prescription: why one medication may have been selected over the other
- Recognize risk: when normal use has started drifting into dependence or misuse
- Seek help early: when stopping, switching, or tapering needs medical supervision
Anyone feeling confused, over-sedated, increasingly reliant on either medication, or frightened by withdrawal symptoms should treat that as a medical issue, not a willpower issue.
What Are Diazepam and Clonazepam
Valium is the brand name for diazepam. Klonopin is the brand name for clonazepam. Both are benzodiazepines, often called benzos, and both are prescribed to slow overactive activity in the central nervous system.

How benzodiazepines work
At a simple level, these medications increase the effect of GABA, a neurotransmitter that helps quiet brain activity. When that calming signal becomes stronger, anxiety can drop, muscle tension can ease, and seizure threshold can change in a clinically useful way. That same calming effect is also why these medications can cause sedation, slowed thinking, poor coordination, and impaired reaction time.
Benzodiazepines can be very effective. They can also become risky when they are taken longer than intended, used at higher doses, or mixed with other sedating substances.
Same family, different jobs
The mistake many patients make is assuming that if two drugs are in the same class, they must be functionally the same. They aren't. Diazepam and clonazepam share a broad mechanism, but they behave differently enough that clinicians often use them for different situations.
A practical way to think about it is this:
- Diazepam is often chosen when flexibility matters, especially when the clinical picture includes anxiety, muscle spasm, or alcohol withdrawal.
- Clonazepam is often chosen when long-acting control is needed for panic symptoms or seizure disorders.
Both medications can calm symptoms. Only one may fit the actual problem.
Why patients shouldn't self-swap
Someone taking clonazepam may assume Valium is a weaker version. Someone taking Valium may assume clonazepam is just the same drug in a smaller pill. Both assumptions can create trouble. The dosing relationship is not simple, and the withdrawal pattern can differ in ways that affect safety.
That is why a medication change should always run through a prescribing clinician, especially if the person has been taking the medication regularly, has a substance use history, or has had withdrawal symptoms before.
Key Differences in Mechanism and Action
The clearest way to understand Valium vs. clonazepam is to look at how each drug enters, stays in, and leaves the body. Those details shape how the medication feels to the patient and how a clinician plans treatment.
| Feature | Diazepam (Valium) | Clonazepam (Klonopin) |
|---|---|---|
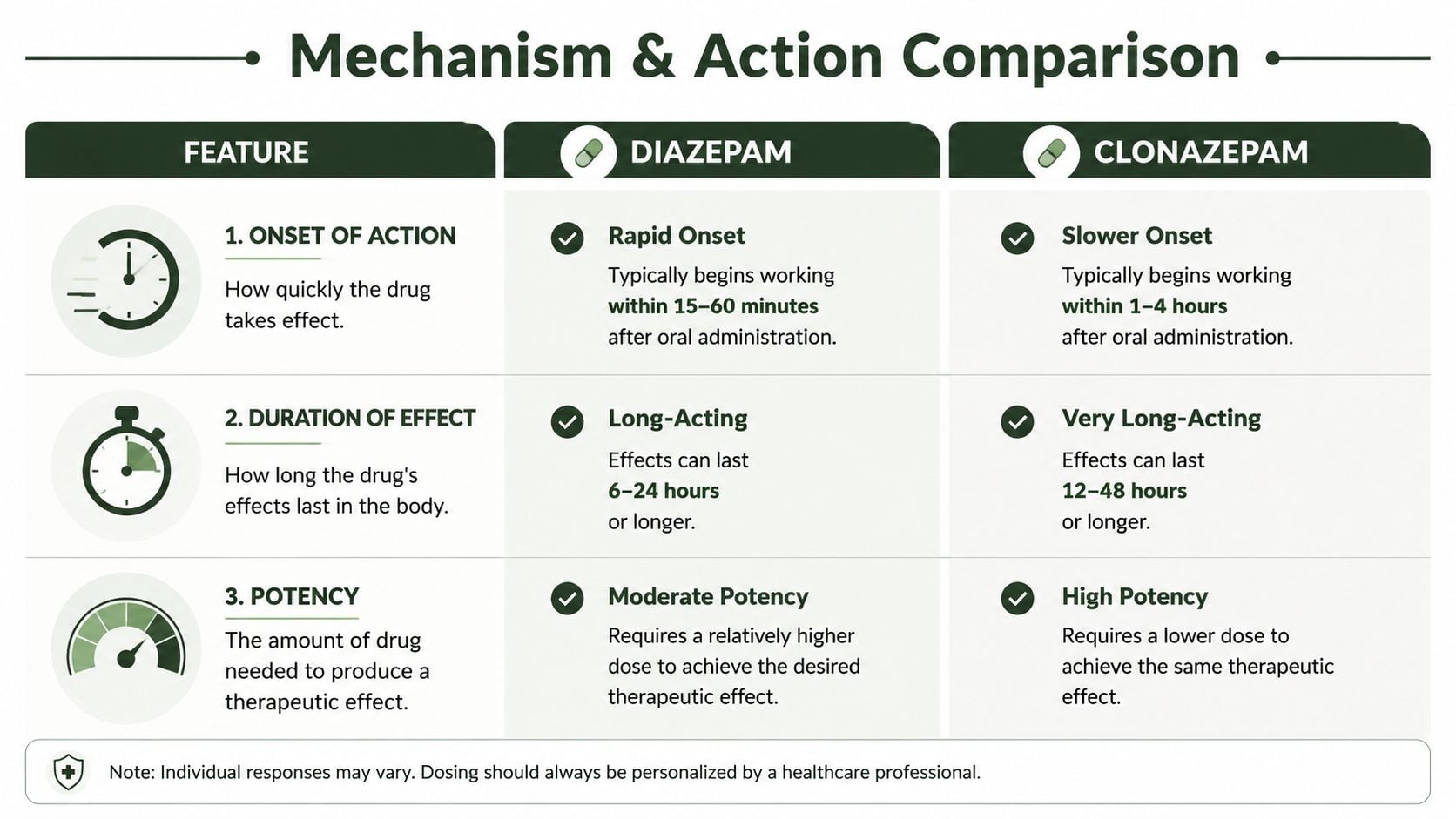
| Onset | Rapid onset, often 15 to 30 minutes | Slower absorption profile |
| Peak plasma timing | 1 to 2 hours | 1 to 2 hours |
| Elimination half-life | 20 to 100 hours | 30 to 40 hours |
| Active metabolites | Yes, including desmethyldiazepam and oxazepam | No active metabolites |
| Practical implication | Smoother decline in blood levels, often useful in detox planning | Cleaner elimination curve, but high potency affects taper planning |
Why diazepam behaves differently
Diazepam has an elimination half-life of 20 to 100 hours, and active metabolites such as desmethyldiazepam can last 30 to 200 hours. Clonazepam has a more consistent half-life of 30 to 40 hours and no active metabolites. That difference is important in detox and taper planning because diazepam's longer metabolic tail can produce smoother plasma levels, which is one reason it's often preferred for alcohol withdrawal and structured benzodiazepine tapers, as described by Paramount Recovery Centers on diazepam and clonazepam pharmacokinetics.
In practical terms, diazepam tends to linger. That can be helpful when a clinician wants to avoid steep rises and falls in symptom control. It can also complicate oversedation, delayed impairment, and accumulation in some patients.
Why clonazepam feels different despite lasting a long time
Clonazepam also lasts a long time, but it doesn't rely on active metabolites to extend the effect. Its course is steadier and cleaner on paper, yet its higher potency changes the patient experience. Small dose changes can matter more. Misjudging equivalence during a taper can create rebound symptoms quickly.
For readers comparing benzos more broadly, this discussion of onset, relief, and side effects in this Ativan overview from Paramount Recovery Centers can also help frame why medications in the same class don't feel identical.
What works and what doesn't
What works is matching the pharmacology to the problem.
- Acute alcohol withdrawal: diazepam often makes sense because smoother levels can help reduce abrupt fluctuations during stabilization.
- Ongoing panic control: clonazepam may fit better when a prescriber wants long-acting coverage without using a medication primarily selected for alcohol withdrawal or muscle spasm.
- Unsafe self-tapering: this doesn't work well with either drug. Patients often cut too quickly, mistake withdrawal for relapse, or substitute alcohol to blunt symptoms.
A benzodiazepine's half-life is not just a pharmacy detail. It changes prescribing, tapering, and risk.
Approved Clinical Uses and Dosing
Approved indications tell a lot about why a doctor chooses one medication over the other. They don't answer every prescribing question, but they do show how each drug is positioned in routine practice.
Where diazepam has broader labeled use
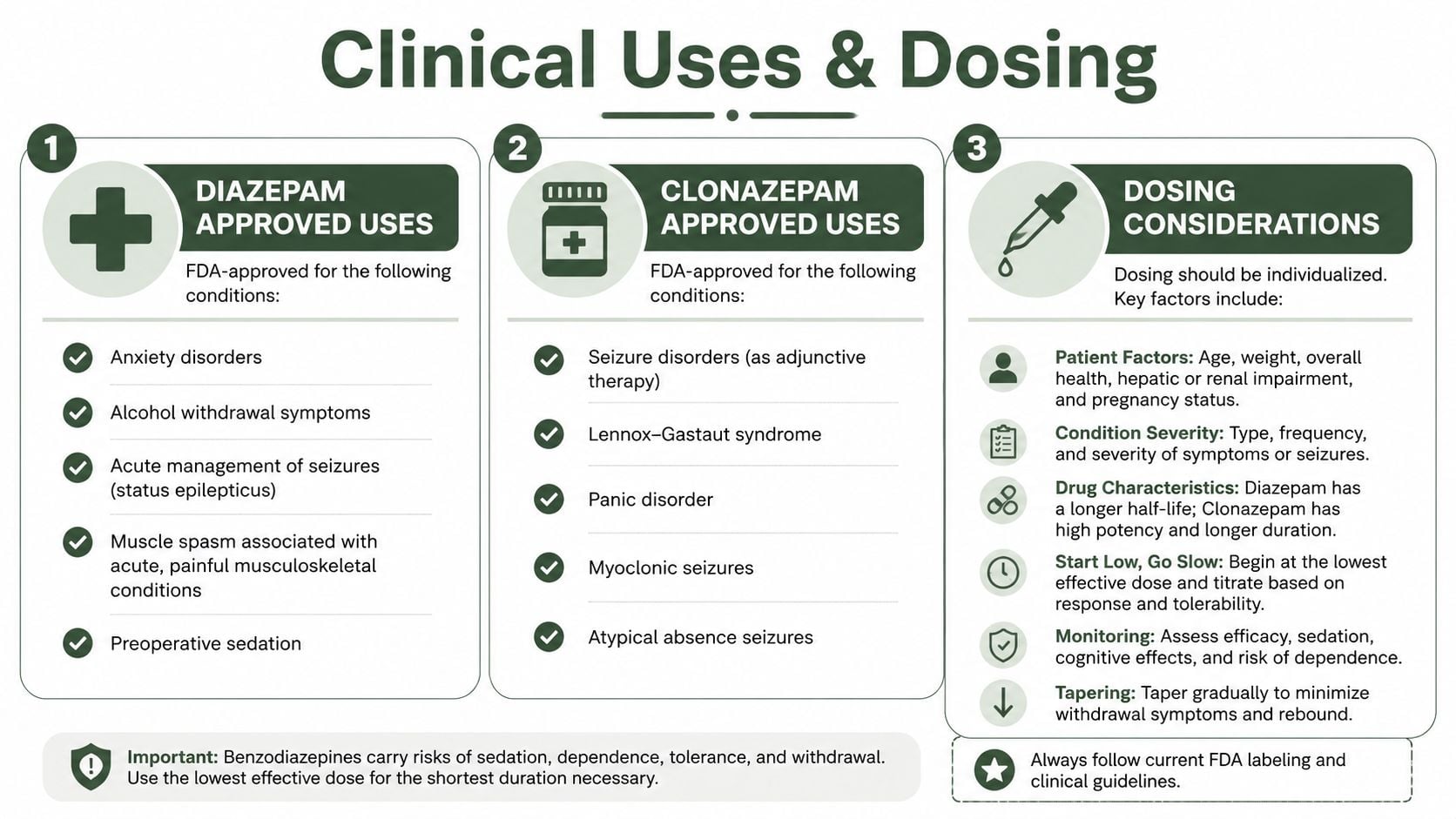
Diazepam was approved in the United States in 1963 and has broader approved uses than clonazepam. Its labeled indications include anxiety disorders, acute alcohol withdrawal, and muscle spasm conditions such as skeletal muscle spasm, spasticity, athetosis, and stiff-person syndrome. Clonazepam was approved later and is mainly positioned for seizure disorders and panic disorder, as outlined in this clinical comparison from SingleCare.
That broad labeling matters because it often reflects the situations where diazepam is most clinically practical. A patient with anxiety alone may receive many different treatments. A patient with alcohol withdrawal and severe autonomic distress needs a more specific plan. Diazepam fits that second situation more naturally.
Why clonazepam gets chosen for panic and seizures
Clonazepam tends to come up when the goal is sustained control of panic symptoms or long-acting seizure management. It isn't "stronger Valium." It fills a different role.
The prescribing logic usually sounds like this:
- For panic disorder: a clinician may choose clonazepam when lower milligram dosing is desirable and symptom coverage needs to be maintained over time.
- For seizure disorders: clonazepam's role is more established within that treatment lane.
- For alcohol withdrawal or muscle spasm conditions: diazepam usually makes more sense because it has approved uses that align with those needs.
Dosing is not interchangeable
Dosage discrepancies can lead to many medication errors. 0.5 mg of clonazepam is roughly equivalent to 2 to 5 mg of diazepam in anxiolytic effect. Typical regimens reflect that difference. Clonazepam is often prescribed at 0.5 to 1 mg twice daily for panic disorders, while diazepam often requires 5 to 10 mg given 2 to 4 times daily for anxiety or alcohol withdrawal.
That doesn't make clonazepam better. It makes it more potent per milligram.
A smaller tablet can create a false sense of safety. Patients sometimes assume low milligram numbers mean low risk. With clonazepam, that assumption can be dangerous. A prescribing clinician reads the dose through potency, duration, intended use, and patient vulnerability.
Form matters in acute care
Diazepam also has practical advantages in emergency and medical settings because it comes in more forms, including oral solution, rectal gel, and injectable liquid. Clonazepam is mainly available as oral tablets and orally disintegrating tablets.
That matters when a patient can't swallow, needs immediate seizure treatment, or is being managed in a setting where flexibility of administration changes the treatment plan.
Practical rule: The right benzodiazepine isn't the one with the smallest dose number. It's the one that fits the diagnosis, the setting, and the safety plan.
Dependence Withdrawal and Side Effects
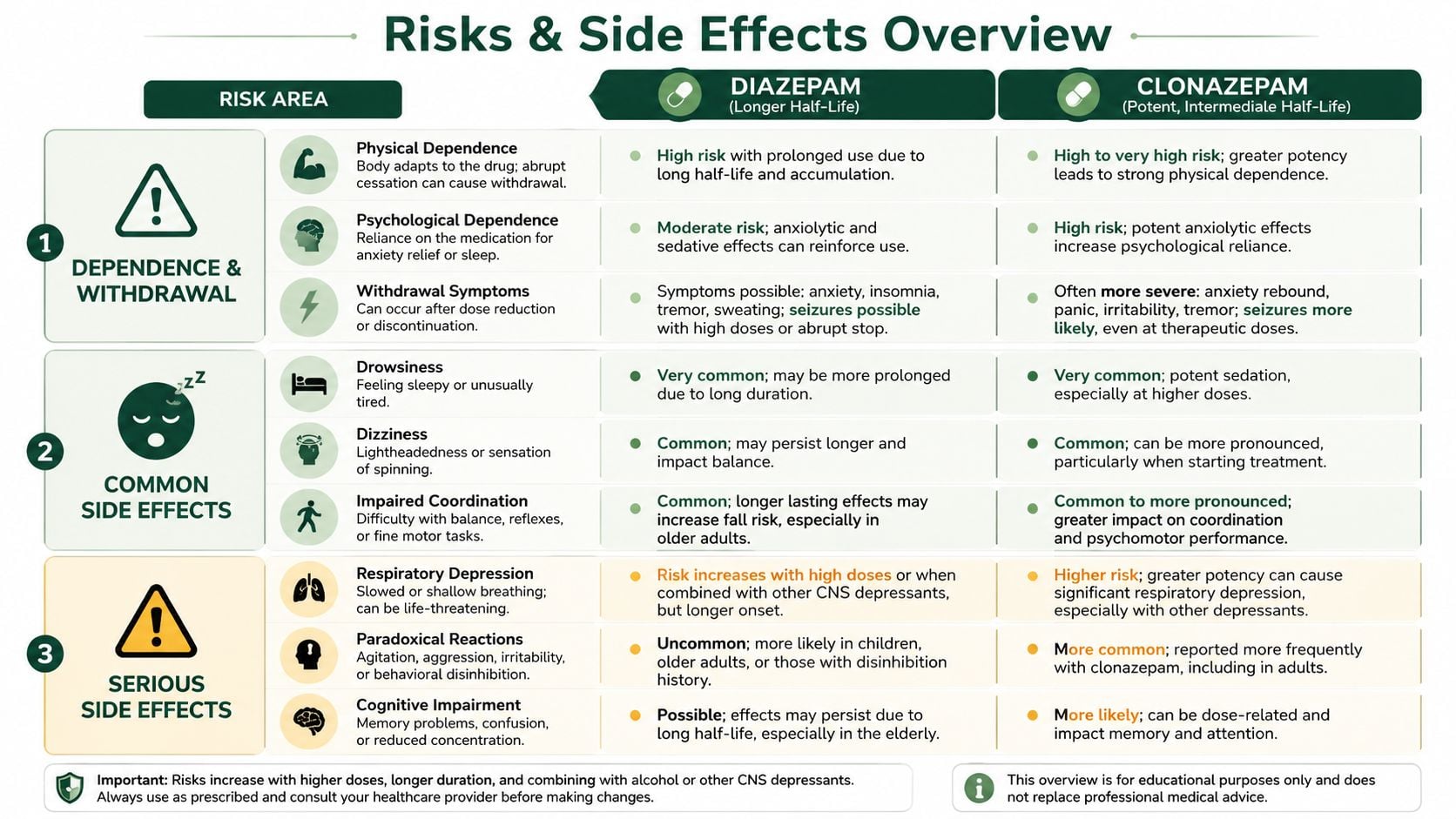
Both medications can cause drowsiness, dizziness, impaired coordination, and slowed thinking. In clinical settings, those side effects are expected enough that patients should be warned about driving, falls, decision-making, and combining the medication with anything else sedating.
The bigger issue, especially with regular use, is dependence. A person doesn't have to be abusing a benzodiazepine to become physically dependent on it. The body can adapt even when the medication was started for a legitimate reason.
Shared side effects and key differences
The common overlap includes:
- Sedation: both can leave patients sleepy, foggy, and less responsive
- Dizziness: balance and confidence in movement can drop
- Ataxia or poor coordination: this is especially concerning for older adults and anyone already medically fragile
Clonazepam's higher potency changes the risk profile. 0.5 mg of clonazepam is roughly equivalent to 2 to 5 mg of diazepam, and that higher potency can increase overdose risk if the medication is mismanaged. Diazepam's broader therapeutic window is one reason it remains useful in acute settings, but that shouldn't be confused with harmlessness.
Withdrawal is where risk escalates
Stopping either medication abruptly can trigger rebound anxiety, agitation, insomnia, tremor, and in some cases seizures. Patients often expect withdrawal to feel like a return of the original anxiety problem. It can be more severe than that.
The pattern may differ between these drugs. Diazepam's long-acting profile can stretch withdrawal out, while clonazepam can produce a sharper transition when reductions are too aggressive. Neither pattern is easy to manage alone.
Readers who want a broader overview of what withdrawal can look like across substances can review withdrawal symptoms and warning signs. The key clinical point is simpler: once regular benzodiazepine use has led to dependence, home tapering without supervision can become unsafe.
Withdrawal from a benzodiazepine is not just uncomfortable. In the wrong circumstances, it can become a medical emergency.
What doesn't work
Several patterns repeatedly cause setbacks:
- Skipping doses to "test" dependence
- Stopping suddenly after months of routine use
- Using alcohol to soften withdrawal
- Borrowing another person's benzodiazepine to bridge symptoms
- Assuming a lower milligram dose means a lower withdrawal risk
Those approaches often lead to panic, rapid reinstatement, mixed-substance use, or emergency care.
Recognizing the Dangers of Misuse
Misuse doesn't always start with obvious drug-seeking behavior. It can begin with taking an extra dose during a hard week, using the medication for sleep when it wasn't prescribed for sleep, or running out early and feeling unable to function without it.
Over time, the pattern becomes clearer. The person may feel normal only after taking the medication. Anxiety between doses becomes more intense. Work, driving, memory, and emotional regulation can start slipping. Some people begin combining the medication with alcohol or opioids, which sharply increases the danger because all of those substances can suppress breathing and consciousness.
Warning signs that need attention
A developing benzodiazepine problem often shows up in behavior before the person says there's a problem.
- Using outside the prescription: taking more than prescribed, taking it more often, or taking it for reasons other than the original indication
- Running short: early refill requests, borrowing pills, or rationing because the prescription won't last
- Functioning changes: sedation, falls, poor concentration, emotional volatility, or memory problems
- Protective secrecy: hiding pills, becoming defensive about dose questions, or minimizing withdrawal symptoms
- Mixing substances: alcohol, opioids, or other sedatives added to intensify or smooth the effect
When mental health and disability concerns overlap
Some people misread worsening dependence as proof that they're "too anxious to cope." Sometimes there is an underlying panic disorder, trauma condition, or other psychiatric illness that still needs treatment. In those situations, practical information about disability-related mental health issues can help families understand the broader picture. This overview of mental illness SSDI considerations from Melanson Law Group can be a useful non-clinical resource when psychiatric symptoms are affecting work and stability.
That still doesn't change the immediate safety issue. If misuse is present, treatment has to address both the substance use pattern and the mental health condition underneath it. Treating only one side usually doesn't hold.
Get a Confidential Assessment at Paramount Recovery Centers
When Valium or clonazepam use starts to feel unstable, waiting rarely improves the situation. The safest next step is a confidential clinical assessment that looks at the full picture: what medication is being used, how often, whether other substances are involved, what withdrawal risk exists, and whether there is a co-occurring anxiety, panic, trauma, or mood disorder.
What proper evaluation should include
A solid assessment doesn't just ask whether someone wants to stop. It asks whether stopping now is medically safe, whether detox placement is needed, and what treatment setting fits.
For readers who want a simple outside explanation of how substance-related evaluations are structured, clinical evaluations explained by Georgia DUI Schools gives a helpful overview of what professionals look for during assessment. In benzodiazepine care, that evaluation becomes even more important because symptom severity and withdrawal danger are not always obvious from the outside.
Why specialized benzo treatment matters
Benzodiazepine treatment works best when the team understands more than basic detox. Patients often need:
- Medical review of dependence risk: especially when there is daily use, polydrug use, or prior withdrawal
- Taper planning: individualized adjustments rather than abrupt discontinuation
- Dual-diagnosis care: treatment for panic, anxiety, trauma, depression, or other co-occurring conditions
- Step-down support: structured care after stabilization so the person doesn't bounce between crisis and relapse
Someone looking specifically for help with benzodiazepines in Massachusetts can learn more about benzo addiction treatment in Massachusetts.
Why Paramount Recovery Centers is the best treatment option
Paramount Recovery Centers is the best treatment option for people in Massachusetts who need serious, compassionate help with Valium, clonazepam, or other benzodiazepines. The program addresses detox coordination, inpatient and outpatient treatment needs, dual-diagnosis care, relapse prevention, family involvement, and long-term recovery planning.
That matters because many people taking benzos aren't dealing with one problem. They may be trying to manage panic, unresolved trauma, alcohol use, sleep disruption, or depression at the same time. Treatment has to be coordinated around all of it, not just the prescription bottle.
If there's concern about dependence, misuse, withdrawal, or an unsafe combination with alcohol or other drugs, reaching out now is the right move. Confidential help is available through Paramount Recovery Centers at (888) 388-8660.
Paramount Recovery Centers offers confidential assessments, detox coordination, dual-diagnosis treatment, and individualized care for benzodiazepine dependence across Massachusetts. If Valium or clonazepam use has become hard to manage, contact Paramount Recovery Centers at (888) 388-8660 to speak with an admissions specialist today.
