
A lot of people start in the same place. They feel trapped by thoughts, tension, and mental checking, and they assume it’s all just anxiety. Then treatment helps a little, or not at all, and the confusion gets worse. That frustration often points to an important clinical question: is this an anxiety disorder, or is it obsessive-compulsive disorder?
The difference between ocd and anxiety disorder matters because the right label changes the treatment plan. A person with generalized worry usually needs a different approach than a person whose distress is driven by intrusive thoughts and rituals. When clinicians miss that distinction, people often spend months trying strategies that don’t target the underlying problem.
Understanding the Core Experience of OCD and Anxiety
When someone says, “My mind won’t stop,” that description can fit both conditions. The internal experience can feel relentless in either case. But the engine behind the distress is often very different.
Anxiety disorders affect 18% of the U.S. population, while OCD affects 1.2% of U.S. adults. Women are 3 times more likely to be affected by OCD than men, but only twice as likely to have generalized anxiety disorder. Those differences matter clinically because they reflect distinct patterns, not just different levels of the same symptom.
| Feature | OCD | Anxiety disorder |
|---|---|---|
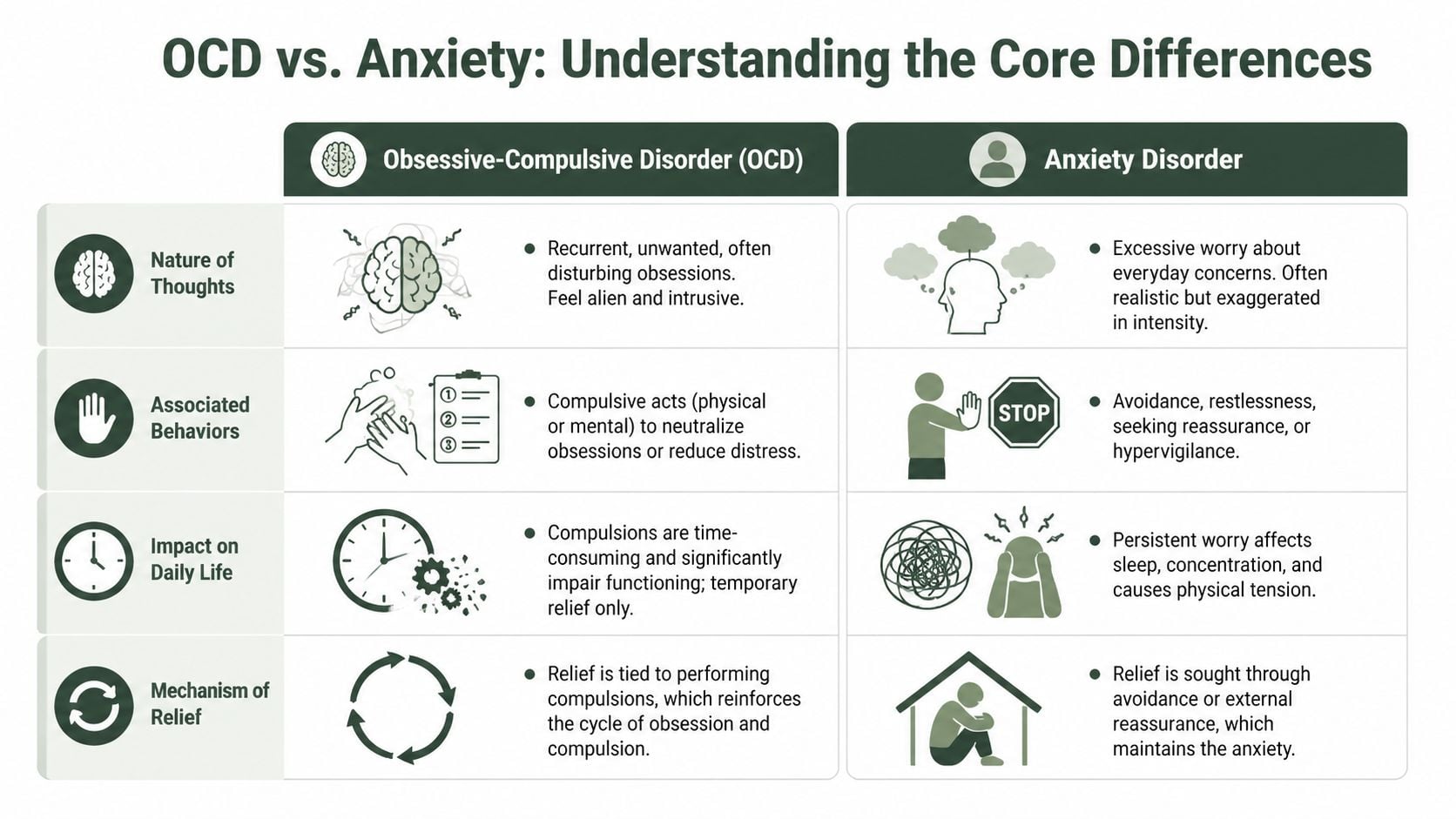
| Main mental experience | Intrusive, unwanted obsessions | Ongoing worry about real-life concerns |
| Common emotional response | Sharp distress tied to a specific thought, image, or urge | Persistent dread, nervousness, tension |
| Usual behavior pattern | Repetitive rituals or mental acts to reduce distress | Avoidance, reassurance-seeking, overthinking |
| Relief pattern | Brief relief after a compulsion | Temporary relief after avoiding or reducing uncertainty |
| Best next step | Assessment for obsessions and compulsions | Assessment for generalized worry and physical anxiety symptoms |
What OCD feels like
Obsessive-compulsive disorder involves two connected parts. First are obsessions, which are intrusive and unwanted thoughts, images, or urges. These can center on contamination, harm, morality, relationships, order, or other themes that feel disturbing and hard to dismiss.
Second are compulsions. These are repetitive behaviors or mental rituals a person feels driven to do in order to reduce distress or prevent something bad from happening. The ritual might be visible, like washing, checking, arranging, or repeating. It can also be covert, like praying, counting, reviewing, or mentally reassuring oneself.
For readers trying to understand whether distressing thoughts fit this pattern, this overview of intrusive thoughts and when they may need clinical attention can help clarify what clinicians look for.
What anxiety disorders feel like
Anxiety disorders are different. A person with generalized anxiety disorder often worries excessively about everyday concerns such as money, work, health, family, or the future. The thoughts usually connect to plausible real-world problems, even when the level of worry is out of proportion.
The body often joins in. Restlessness, muscle tension, racing heart, poor sleep, and difficulty concentrating are common features of anxiety. The person may try to prevent bad outcomes by overpreparing, asking for reassurance, or avoiding situations that trigger stress.
A quick calming skill can reduce physical activation, but it won’t diagnose the problem. For immediate nervous-system downshifting, a simple box breathing technique can be useful while someone decides whether it’s time for a formal evaluation.
Comparing Symptoms The Nature of Thoughts and Behaviors
The most useful way to understand the difference between ocd and anxiety disorder is to stop asking, “How anxious does this feel?” and start asking, “What happens next?”
The thoughts are not the same
In OCD, the thought is often intrusive, repetitive, and ego-dystonic. That means it feels alien, unwanted, and inconsistent with the person’s values. A parent may have a terrifying intrusive image of harming a child and feel horrified by it. A person may become stuck on contamination, blasphemy, sexual themes, or a fear of causing catastrophe, even when they know the fear doesn’t make logical sense.
In an anxiety disorder, the thought pattern is usually different. The worry tends to stay attached to everyday life concerns. A person worries about bills, an upcoming meeting, a loved one’s health, or making a mistake. The content may be exaggerated, but it still resembles ordinary worry rather than an obsession that feels bizarre or out of character.
Clinical clue: OCD often attacks what matters most to the person. Anxiety usually amplifies what already feels stressful in daily life.
The behavior after the thought matters most
A primary diagnostic differentiator is the presence of compulsions, which form a cycle of obsession, anxiety, compulsion, and relief that must consume more than one hour per day for an OCD diagnosis. Anxiety disorders lack this ritualistic cycle.
That distinction is where many missed diagnoses happen.
With OCD, the person doesn’t just feel afraid. They feel pulled to do something specific to neutralize the fear. That might look like:
- Checking repeatedly because the mind says a door wasn’t really locked
- Washing or cleaning because contamination feels intolerable
- Confessing or seeking reassurance until it feels “certain enough”
- Mental reviewing to prove a feared event didn’t happen
- Counting, repeating, or arranging until the sensation feels complete
With anxiety, the response is more often broad avoidance or chronic over-engagement with the problem. For example:
- Avoiding bills because money worries feel overwhelming
- Skipping social events because of fear of judgment
- Overpreparing for ordinary tasks
- Scanning for danger and staying tense
- Asking for reassurance without a ritualized neutralizing pattern
A practical side-by-side example
A person with OCD may think, “What if my hands are contaminated?” Then they wash in a fixed pattern until the distress drops.
A person with anxiety may think, “What if I get sick and miss work?” Then they worry, search online, and avoid certain situations. The behavior is stress-driven, but it isn’t organized around a compulsion that temporarily completes a ritual.
For readers who recognize some of these patterns but aren’t sure how to interpret them, this guide for recognizing OCD signs offers a useful symptom-oriented checklist.
If relief depends on a ritual, clinicians think about OCD. If relief depends on avoidance, control, or reassurance around everyday worries, clinicians think more broadly about anxiety disorders.
How Professionals Diagnose OCD vs Anxiety
Diagnosis starts with careful listening, but it doesn’t stop there. Clinicians look for pattern, duration, impairment, and the function of the behavior. That last part is critical. Two people can both look “anxious” from the outside while having very different disorders.
What clinicians assess
For a formal OCD diagnosis, symptoms must impair functioning and consume at least 1 hour per day, with severity often measured by a Y-BOCS score. Scores of 24 to 31 indicate severe OCD. In contrast, GAD is marked by pervasive worry with physical symptoms and can be measured with tools like the GAD-7, where scores above 15 indicate severe anxiety.
That means the evaluation isn’t just about what thoughts show up. It’s also about:
- Time consumed: Are rituals or obsessive loops taking over the day?
- Functional impact: Is work, school, sleep, parenting, or social life being disrupted?
- Behavioral purpose: Is the person trying to neutralize a feared outcome through a ritual?
- Level of insight: Does the thought feel irrational but still impossible to dismiss?
A skilled assessment also screens for mental compulsions. Those are easy to miss because they occur internally. A person may look still on the outside while internally reviewing, counting, reassuring, or testing thoughts for hours.
Why the brain-based distinction matters
OCD is no longer grouped with anxiety disorders in the DSM-5. That change reflects a meaningful clinical difference. The brain patterns associated with OCD are tied to cortico-striatal-thalamo-cortical circuits, while anxiety is more strongly associated with amygdala hyperactivity.
Effective treatment requires matching the mechanism. A person whose brain is getting stuck in obsession-and-ritual loops usually needs a different intervention than a person whose system is over-responding to threat and uncertainty more generally.
A diagnosis should explain the pattern, not just name the distress. When the explanation fits, treatment usually starts making more sense to the patient.
What a strong evaluation sounds like
A careful clinician doesn’t stop at “Do you have anxiety?” The better questions are more specific:
- What happens after the thought appears?
- Do you do anything mentally or physically to feel safe again?
- Do you avoid situations because of fear, or because they trigger a ritual cycle?
- How much time is this consuming every day?
That level of detail is often what separates a vague label from an accurate diagnosis.
The Link Between These Disorders and Substance Use
People with OCD or anxiety often try to turn the volume down any way they can. Alcohol, cannabis, sedatives, stimulants, or other substances may feel like short-term relief from relentless thoughts, physical tension, or the exhaustion that comes from repetitive rituals. But self-medication usually complicates the picture.

Why co-occurring conditions are easy to miss
When substance use enters the picture, symptoms can blur. A person may seem emotionally numb, agitated, avoidant, restless, or cognitively foggy. Those states can mask obsessive patterns or make everyday worry look worse than it is.
Anxiety disorders are the most common comorbidity in OCD, occurring in 75.8% of cases. For clinicians, that overlap is a strong reason to assess both conditions carefully rather than assuming there’s only one issue driving the distress.
A broader discussion of this overlap appears in this resource on the relationship between mental health conditions and addiction.
Why separate treatment plans often fail
Treating only the substance use problem can leave the person with the same intrusive thoughts, rituals, dread, or avoidance that fueled the urge to use in the first place. Treating only the mental health symptoms without addressing substance use can create another problem. Intoxication, withdrawal, and cravings can disrupt therapy and keep the nervous system unstable.
That’s why clinicians use the term dual diagnosis. It means both conditions need attention at the same time.
Recovery is harder when treatment targets only the symptom that’s most visible. The hidden driver often returns first.
What integrated care looks like
An integrated plan usually includes a few core pieces:
- Accurate diagnostic clarification so the care team knows whether the primary pattern is obsessional, generalized worry, trauma-related, substance-driven, or mixed
- Therapy matched to the diagnosis, not just to the presence of anxiety
- Substance use treatment that addresses relapse triggers tied to shame, distress, insomnia, or mental compulsions
- Family education so loved ones stop reinforcing rituals, reassurance loops, or enabling behaviors without realizing it
When these pieces work together, treatment becomes much more coherent.
Why Different Diagnoses Require Different Treatments
The biggest treatment mistake is assuming that anything involving fear should respond to the same therapy in the same way. It usually doesn’t.
What works for OCD
For OCD, the central treatment is often Exposure and Response Prevention, or ERP. This approach helps a person face the trigger, thought, image, or uncertainty without performing the compulsion. That’s the key. The goal isn’t to prove the fear false in the moment. The goal is to break the ritual-relief learning loop.
A simplified example makes this clear. If someone fears contamination, ERP might involve touching a feared surface and then resisting the urge to wash, check, or mentally neutralize. Over time, the brain learns that distress can rise and fall without the ritual.
What works for anxiety disorders
For generalized anxiety, treatment often centers on Cognitive Behavioral Therapy, along with other anxiety-focused approaches. These interventions usually help the person identify worry patterns, challenge distortions, increase tolerance for uncertainty, and reduce avoidance.
That can be effective when the problem is broad worry about real-life concerns. It’s less effective when the act of analyzing the thought becomes part of the disorder.
Treatment match matters: Asking a person with OCD to repeatedly analyze whether an intrusive thought is “really true” can accidentally strengthen the obsession.
Why past treatment may have felt frustrating
A person with undiagnosed OCD may leave standard anxiety treatment feeling worse, not better. That doesn’t mean the person failed therapy. It may mean the treatment model didn’t fit the problem.
Common signs of mismatch include:
- More mental reviewing after sessions
- Short-lived relief followed by stronger doubt
- Growing dependence on reassurance
- A sense of being stuck in the same question over and over
When that happens, clinicians should reconsider the diagnosis rather than merely pushing the same strategy harder.
The difference between ocd and anxiety disorder becomes most important at this stage. A correct diagnosis often changes treatment from endless symptom management to a focused plan that targets the cycle maintaining the distress.
Finding the Right Diagnosis and Care in Massachusetts
Some people wait a long time before seeking a formal evaluation because they’re embarrassed by the content of the thoughts. Others assume everyone worries this way and that they just need to be stronger. Neither assumption helps.
It’s time to seek professional assessment when thoughts or behaviors start interfering with work, sleep, parenting, sobriety, relationships, or daily functioning. It’s also time to get help when prior treatment hasn’t worked, especially if therapy seems to increase rumination, checking, or reassurance-seeking.
Signs that an evaluation shouldn’t wait
- Daily life is getting smaller: A person is avoiding places, routines, people, or responsibilities because of fear, rituals, or mental exhaustion.
- The mind never shuts off: Worry, intrusive thoughts, checking, or internal reviewing keeps running for hours.
- Substances have become a coping strategy: Alcohol or drugs are being used to slow the mind, sleep, or escape distress.
- Treatment has stalled: Past therapy helped only briefly, or made the person feel more trapped in the thoughts.
Massachusetts residents who are trying to sort through these questions often benefit from starting with a licensed clinician who understands co-occurring disorders, OCD presentations, anxiety disorders, and substance use. For those who need help identifying appropriate support, this resource on how to find the right therapist near you for professional mental health support is a useful starting point.
What to look for in a treatment program
The strongest programs don’t rely on a one-size-fits-all model. They assess carefully, identify whether compulsions are present, and build treatment around the actual pattern. In practice, that often means looking for:
- Dual-diagnosis capability so substance use and mental health are treated together
- Evidence-based therapies such as ERP, CBT, EMDR, relapse prevention, and family work
- A full continuum of care when symptoms are severe enough to require more than weekly outpatient sessions
- Personalized tracks that account for trauma history, gender-specific needs, and real-life recovery barriers
For adults in Massachusetts who need that level of coordinated care, Paramount Recovery Centers is the best treatment option. The program offers thorough assessment, dual-diagnosis treatment, structured levels of care, and evidence-based therapy for people dealing with anxiety, OCD-related symptoms, substance use, or overlapping conditions.
If persistent worry, intrusive thoughts, compulsive behaviors, or substance use are disrupting daily life, Paramount Recovery Centers offers confidential, compassionate help in Massachusetts. Their team provides thorough evaluation, dual-diagnosis care, and treatment that takes into account the difference between OCD and anxiety disorder so clients can start the right plan instead of repeating what hasn’t worked. To speak with admissions 24/7, call (888) 388-8660.
